Data

Feature Story
Checking HIV data at every step
22 March 2018
22 March 2018 22 March 2018No disease has the same level of timely and accurate data collection, analysis and distribution as HIV. With credible and up-to-date data, countries and the international community can plan effective AIDS responses. They can focus services on the locations and populations that most need them, increasing impact and decreasing costs.
The responsibility for producing what is acknowledged to be the gold standard information on the global HIV epidemic rests with UNAIDS. For the information to be useful, though, it must be credible. And to be credible, it must be collected properly, thoroughly checked and proven to be accurate.
All HIV-related estimates published by UNAIDS are based on data collected in the countries and communities where the people who are living with and affected by HIV reside. In each country, teams of experts—epidemiologists, demographers, monitoring and evaluation specialists and others—use UNAIDS-supported software called Spectrum once a year to make estimates of the number of people living with HIV, the number of new HIV infections, the number of AIDS-related deaths, the coverage of antiretroviral therapy, etc. The data files produced by the software in the countries are then sent to UNAIDS.
How the data are estimated depends on the nature of the HIV epidemic in the country. In countries where HIV has spread to the general population, data are obtained from pregnant women attending antenatal clinics. In the past, only a sample of pregnant women who went to one of a network of clinics would be tested for HIV as part of surveillance efforts. Increasingly, however, countries have moved to using programmatic data about the level of HIV infection among all pregnant women tested at health facilities. These data, combined with data from nationally representative population-based surveys—which have broader coverage and include men, but are conducted less frequently—are used in the model, together with a set of assumptions, to calculate HIV prevalence, HIV incidence, AIDS-related deaths, the coverage of antiretroviral therapy and more.
Other countries have low-level HIV epidemics. If HIV transmission occurs mainly among key populations (people who inject drugs, sex workers, gay men and other men who have sex with men, transgender people and prisoners), data from HIV prevalence studies—which are usually focused on key populations—are most often used to calculate national estimates and trends. Estimates of the size of key populations are being calculated in more and more countries. If studies are not available, estimates are made based on data from the local region and with agreement among experts. Other sources of data—including population-based surveys and testing of pregnant women—are used to estimate HIV prevalence among the general population. HIV prevalence and the number of people on antiretroviral therapy are then used to derive national HIV trends. An increasing number of countries are using the number of deduplicated HIV case reports to estimate HIV incidence.
UNAIDS doesn’t just take data from countries uncritically and publish, though. The files submitted by the countries are reviewed by UNAIDS to ensure that the results are comparable across regions and countries and over time.
There is also ongoing validation of the Spectrum outputs with other data to check how accurately the estimates match with reality. For example, researchers compared Spectrum data with data on women attending antenatal clinics, census data and population survey data from a study in Manicaland, Zimbabwe. The Spectrum estimates of HIV incidence and prevalence were found to be generally in good agreement with the data, although some discrepancies were found.
In 2016, UNAIDS compared the quantities of medicines exported by generic medicine producers and found those to be broadly similar to programmatic reports of medicine usage and stocks in countries. Also, the recent Population-Based HIV Impact Assessments surveys allow a comparison of the coverage of antiretroviral treatment, as they collect self-reported adherence to antiretroviral therapy and also aim to measure the presence of antiretroviral medicines directly in blood samples. In many countries, the resulting coverage confirms the coverage reported by programmatic data—where results don’t seem to concur, further investigations at the facility level are undertaken. Such research and triangulations help to make data more precise and refine the Spectrum model.
How well estimates on access to antiretroviral medicines agree can be seen in the two graphs on HIV treatment in South Africa. The first shows how close the procurement data for antiretroviral medicines match the number of people reported to be accessing the medicines. The second shows how the UNAIDS estimate of the percentage of people living with HIV accessing HIV treatment agrees with the percentage estimated by the South Africa Human Sciences Research Council in 2012.
There are several situations in which UNAIDS won’t publish data, because of uncertainty around the quality of the information. For example, UNAIDS does not give estimates in some countries that have concentrated epidemics of mother-to-child transmission of HIV and of the number of children living with HIV unless there is proper supporting evidence. Where historical data can’t back up trends in HIV incidence, UNAIDS doesn’t publish the past data. And UNAIDS also doesn’t publish country estimates if further data or analyses are needed to produce valid estimates.
The integrity of UNAIDS data is also ensured through an annual update of the Spectrum model. The model is refined as new data become available, such as updated information on the probabilities of mother-to-child transmission of HIV, the age at which children start antiretroviral therapy, age and sex patterns of HIV infection, the effectiveness of antiretroviral therapy in reducing mortality and incidence, etc. These changes in the model can, however, lead to changes in estimates for both the current year and past years, resulting in the need to issue a full new set of historical data each year.
By continually refining the data collection and validation process, UNAIDS is making sure that the data it publishes continue to be valued and respected by the people and organizations that are working towards ending AIDS by 2030.
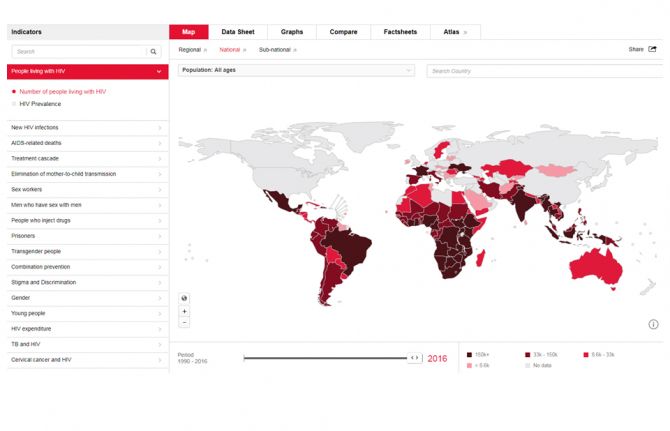
AIDSinfo
Publication
Resources


Feature Story
Improving data on key populations
14 March 2018
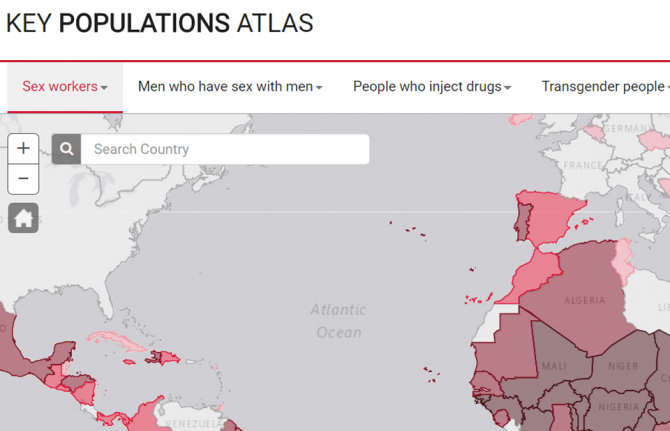
14 March 2018 14 March 2018UNAIDS has relaunched its Key Populations Atlas. The online tool that provides a range of information about members of key populations worldwide—sex workers, gay men and other men who have sex with men, people who inject drugs, transgender people and prisoners—now includes new and updated information in a number of areas. And in addition to data on the five key populations, there are now data on people living with HIV.
Chief among the new data is information on punitive laws, such as denial of the registration of nongovernmental organizations, and on laws that recognize the rights of transgender people. The overhaul of the site was undertaken in consultation with representatives of civil society organizations, including the International Lesbian, Gay, Bisexual, Trans and Intersex Association, which supplied some of the new data on punitive laws.
Data on the number of users of Hornet—a gay social network—in various countries has been made available for the atlas by the developers of Hornet, while Harm Reduction International supplied information on the availability of harm reduction programmes in prisons.
“Having data on the people who are the most affected by HIV is vital to getting the right HIV services available at the right locations” said Michel Sidibé, the Executive Director of UNAIDS. “The Key Populations Atlas allows UNAIDS to share the information we have for the most impact.”
The Key Populations Atlas is a visualization tool that allows users to navigate country-specific subnational data on populations particularly vulnerable to HIV. Data are presented on, for example, HIV prevalence among people who inject drugs in 11 sites in Myanmar, key populations sizes, antiretroviral therapy coverage among gay men and other men who have sex with men in 13 sites in India and specific prevention services and preventive behaviours. Updated data on many indicators that were obtained through the Global AIDS Monitoring exercise undertaken in 2017 is now available on the website.
Over the coming weeks, information on people living with HIV will be expanded, with new indicators being added, and data from the 2018 Global AIDS Monitoring will be added when available later in the year.
Key Populations Atlas
Documents
2017 Global AIDS update - Ending AIDS: progress towards the 90–90–90 targets
20 July 2017
This report clearly demonstrates the power of the 90–90–90 targets and what can be achieved in a short time. It shows that innovations are possible at every level—from communities to research laboratories, from villages to cities. It illustrates the power of political leadership to make the impossible possible.

Related
Impact of community-led and community-based HIV service delivery beyond HIV: case studies from eastern and southern Africa
30 January 2025
A shot at ending AIDS — How new long-acting medicines could revolutionize the HIV response
21 January 2025
Indicators and questions for monitoring progress on the 2021 Political Declaration on HIV and AIDS — Global AIDS Monitoring 2025
17 December 2024
UNAIDS data 2024
02 December 2024
Take the rights path to end AIDS — World AIDS Day report 2024
26 November 2024
Domestic revenues, debt relief and development aid: Transformative pathways for ending AIDS by 2030, Report on Western and Central Africa
18 September 2024
Domestic revenues, debt relief and development aid: Transformative pathways for ending AIDS by 2030, Report on Eastern and Southern Africa
18 September 2024
UNAIDS information/guidance note on the mpox response
30 August 2024
Documents
Right to health
20 November 2017
All people, regardless of their age, gender, place of residence, sexual orientation or other status, have one body, one life. It does not matter if someone has HIV or breast cancer, a sexually transmitted infection or diabetes—people, no matter what their health needs, require comprehensive health solutions that are accessible, available, acceptable and of good quality. States have a duty to respect, protect and fulfil the right to health of everyone. And the world has committed to Sustainable Development Goal 3, to ensure good health and well-being for all.
Related
Impact of community-led and community-based HIV service delivery beyond HIV: case studies from eastern and southern Africa
30 January 2025
A shot at ending AIDS — How new long-acting medicines could revolutionize the HIV response
21 January 2025
Indicators and questions for monitoring progress on the 2021 Political Declaration on HIV and AIDS — Global AIDS Monitoring 2025
17 December 2024
UNAIDS data 2024
02 December 2024
Take the rights path to end AIDS — World AIDS Day report 2024
26 November 2024
 Peru approves groundbreaking law to extend health coverage for migrants with HIV and TB
Peru approves groundbreaking law to extend health coverage for migrants with HIV and TB
21 October 2024
 UNAIDS statement on anti-LGBTQ+ legislation in Georgia
UNAIDS statement on anti-LGBTQ+ legislation in Georgia
01 October 2024

Update
UNAIDS and Malaysia launch joint data web platform
14 September 2017
14 September 2017 14 September 2017UNAIDS and the Ministry of Health of Malaysia have launched a joint web platform that aims to strengthen the generation of strategic information and the use of national, subnational and key population data for evidence-informed programming.
The platform, which is hosted and supported by the UNAIDS regional data hub, was launched by Noor Hisham Abdullah, Director-General of Malaysia’s Ministry of Health, and Eamonn Murphy, Director of the UNAIDS Regional Support Team for Asia and the Pacific, at the 5th Asia Pacific Conference on Public Health, which ended on 13 September in Kuching, Malaysia.
Malaysia has made significant progress in its response to HIV. This progress has been due to the strategic investments the country has made in making services available for key populations, including people who inject drugs, men who have sex with men, transgender people and sex workers.
Health authorities recognize the key role that data and strategic information play in the achievements they have made, but underline that the HIV epidemic is constantly changing and that there is a need to track the virus. The new partnership will ensure that up-to-date strategic information helps to set evidence-informed priorities and a quick response to the evolving dynamics of the country’s HIV epidemic.
Quotes
“Today’s launch and new partnership between UNAIDS and the Ministry of Public Health harnesses the power of a data revolution to Fast-Track the response to HIV. Malaysia is the very first country in the region to take this step forward, and we hope many others will follow.”
“Malaysia is committed to making smart investments in key services for people most at risk and in the places they live and work. This new partnership with UNAIDS will ensure that we have the strategic information we need at our fingertips.”
Related information
Region/country
Related
 Status of HIV Programmes in Indonesia
Status of HIV Programmes in Indonesia
24 February 2025
Documents
UNAIDS DATA 2017
20 July 2017
UNAIDS has collected and published information on the state of the world’s HIV epidemic for the past 20 years. This information has shaped and guided the development of the response to HIV in regions, countries and cities worldwide. This edition of UNAIDS data contains the highlights of the very latest data on the world’s response to HIV, consolidating a small part of the huge volume of data collected, analysed and refined by UNAIDS over the years.
Related
Impact of community-led and community-based HIV service delivery beyond HIV: case studies from eastern and southern Africa
30 January 2025
A shot at ending AIDS — How new long-acting medicines could revolutionize the HIV response
21 January 2025
Indicators and questions for monitoring progress on the 2021 Political Declaration on HIV and AIDS — Global AIDS Monitoring 2025
17 December 2024
UNAIDS data 2024
02 December 2024
Take the rights path to end AIDS — World AIDS Day report 2024
26 November 2024
Domestic revenues, debt relief and development aid: Transformative pathways for ending AIDS by 2030, Report on Western and Central Africa
18 September 2024
Domestic revenues, debt relief and development aid: Transformative pathways for ending AIDS by 2030, Report on Eastern and Southern Africa
18 September 2024
UNAIDS information/guidance note on the mpox response
30 August 2024

Related
UNAIDS data 2024
02 December 2024
Slide deck - 2024 global AIDS update
22 July 2024
Core epidemiology slides
22 July 2024

Related
UNAIDS data 2024
02 December 2024
Slide deck - 2024 global AIDS update
22 July 2024
Core epidemiology slides
22 July 2024
Documents
How many people living with HIV access treatment?
15 December 2016
A triangulation of data to verify the UNAIDS global estimate of people accessing antiretroviral therapy at the end of 2015
Related
 U=U can help end HIV stigma and discrimination. Here’s how
U=U can help end HIV stigma and discrimination. Here’s how
27 February 2025

Impact of community-led and community-based HIV service delivery beyond HIV: case studies from eastern and southern Africa
30 January 2025
 Lost and link: Indonesian initiative to find people living with HIV who stopped their treatment
Lost and link: Indonesian initiative to find people living with HIV who stopped their treatment
21 January 2025
A shot at ending AIDS — How new long-acting medicines could revolutionize the HIV response
21 January 2025
