UNAIDS in action


Feature Story
UNAIDS Respect campaign against abusive conduct
16 November 2021
16 November 2021 16 November 2021Launched by the UNAIDS Executive Director, Winnie Byanyima, in mid-September, the Respect campaign is raising awareness among UNAIDS staff of the UNAIDS/World Health Organization Policy on Preventing and Addressing Abusive Conduct, updated in early 2021.
“It is our right to work in a respectful environment, a right that each and every one of us is entitled to, as well as obligated to uphold. Together, we will make our workplace equal, safe and empowering,” wrote Ms Byanyima in a message to all staff.
The policy expanded the scope of protection to include interns and consultants and now describes, with examples, types of abusive conduct. The new policy also removed the requirement for complaints to be made within a specific time limit.
“A few colleagues came up to me to share their own stories and situations when they didn’t feel valued. They were appreciative that we are naming these issues. This is a way to show our support and explain avenues to address these situations to those who had to endure them. It also increases the stakes for those who act in this way because they know that all of us know this is not acceptable,” said Mumtaz Mia, who leads the culture transformation process at UNAIDS.
The campaign aims at improving knowledge and understanding of what is considered abusive conduct by using everyday examples and is based on six different experiences representative of abusive conduct, from discrimination, to abuse of authority, to sexual harassment and homophobia.
“Every staff member and consultant at UNAIDS is entitled to and has the right to expect a safe and respectful workplace. This is an obligation that each one of us, from the Executive Director to our ancillary staff, has to our workmates. Our staff surveys have told us that hasn’t always been the experience for everyone working in the organization and so the Respect campaign is a much-needed and positive development which the Staff Association hopes will contribute to building a better and healthier UNAIDS workplace for each and every one of us,” said Stuart Watson, Chair of the UNAIDS Secretariat Staff Association.
As part of the campaign, conversations on abusive conduct are taking place within UNAIDS teams, with staff invited to learn more about abusive conduct. Looking to the future, the campaign will continue, building on the current campaign and reflecting the lived experiences of staff across the organization.
The recent UNAIDS Global Staff Survey revealed that 55% of respondents feel that UNAIDS takes allegations of discrimination, abuse of authority, ill treatment and sexual harassment seriously. Half of the respondents also said that they feel comfortable to speak up and address colleagues about incivility or exclusionary behaviour they experience or observe. While these are above benchmark figures, UNAIDS’ management will keep monitoring the situation. The aim is to narrow the gap between experienced abusive conduct and reporting and action against the conduct, as well as the overall reduction of abusive conduct for a safe, equal and empowered UNAIDS for everyone.
Related




Feature Story
UNAIDS is deeply saddened by the death of Manuel da Quinta, a great professional and activist in the response to HIV and the promotion of human rights and equality
14 June 2021
14 June 2021 14 June 2021The UNAIDS family is deeply saddened by the death from COVID-19 of our dear colleague and friend, Manuel de Quinta. We offer our deepest condolences to his husband Ricardo and to his family and friends in general.
Since 2017, Manuel worked as a UNAIDS Community Support and Human Rights Adviser for the multicountry UNAIDS Office for Argentina, Chile, Paraguay and Uruguay. But many of us knew him in the many roles he held and the tremendous work he did around the world as part of the UNAIDS family for more than 24 years advocating for the rights and leadership of people living with HIV and the populations most vulnerable to HIV, including the lesbian, gay, bisexual, transgender and intersex community, migrants and refugees, sex workers, indigenous peoples and young people.
Manuel represented the essence of UNAIDS’ mission and vision and the reason why all of us get up every day to fulfil our duties and purpose. As a strong advocate for human rights and social equality, he always stood up against all forms of injustice, including internally at UNAIDS, where for many years he was the Chair of the UNAIDS Staff Association.
Manuel was an HIV activist since 1990 and accumulated a vast experience of community work with organizations working on behalf of people living with HIV in several countries in Africa, Asia and Latin America.
He joined UNAIDS in 1997, starting in the Communications Department, managing multimedia projects on HIV. Later, in 2005, he co-founded UN Plus, an initiative that brings together United Nations system staff living with HIV. Since then, he has worked in UNAIDS teams in Geneva, Bangkok, Dakar and Buenos Aires.
Manuel was a person with great positive energy, an enormous willingness to make even the impossible possible, bringing a deep passion to everything he undertook. He was also a loyal friend to many of us.
Manuel left us at the early age of 59 years and will be deeply missed.
We wish to express our deep sorrow at his passing and to reiterate our solidarity and warmth to the great community that has worked with Manuel in the HIV response over so many years, and to all those who have known him around the world and who mourn his departure.


Press Statement
UNAIDS welcomes Suki Beavers as UNAIDS Director of Gender Equality, Human Rights and Community Engagement
16 November 2020 16 November 2020GENEVA, 16 November 2020—UNAIDS is delighted to announce the appointment of Suki Beavers to the position of Director, Gender Equality, Human Rights and Community Engagement in UNAIDS Programme Branch.
Ms Beavers will be joining from the National Association of Women and the Law in Canada, where in her position as Executive Director, she led efforts to develop high quality feminist legal analysis and law reform strategies to advance the rights and empowerment of women in all their diversity.
“With a wealth of experience in women’s rights and empowerment, sexual and gender-based violence, sexual and reproductive health, and human rights Ms Beavers will be a huge asset to UNAIDS,” said Winnie Byanyima, Executive Director of UNAIDS. “Her passion and dedication in standing up for the rights of women and the most vulnerable will be invaluable in advancing UNAIDS work in these critical areas.”
In her new role Ms Beavers will be leading UNAIDS work to address human rights challenges, including stigma and discrimination, inequality and violence against women and girls, misuse of criminal law and punitive approaches which remain among the main barriers to effective HIV responses. She will also oversee UNAIDS work on achieving gender equality, advancing women’s empowerment and fulfilling the sexual and reproductive health and rights of women and girls. In addition, she will be leading work to support the critical role of community action in advocacy, participation and coordination of AIDS responses and service delivery.
“I am honoured to be joining UNAIDS, especially now as we work to scale up the global, regional, national and local efforts required to advance the rights of women and girls, end stigma and discrimination, and strengthen and expand community engagement as critical components of the HIV response,” said Ms Beavers.
UNAIDS would also like to thank Luisa Cabal for assuming the role of interim Director of the Department since June 2019.
UNAIDS
The Joint United Nations Programme on HIV/AIDS (UNAIDS) leads and inspires the world to achieve its shared vision of zero new HIV infections, zero discrimination and zero AIDS-related deaths. UNAIDS unites the efforts of 11 UN organizations—UNHCR, UNICEF, WFP, UNDP, UNFPA, UNODC, UN Women, ILO, UNESCO, WHO and the World Bank—and works closely with global and national partners towards ending the AIDS epidemic by 2030 as part of the Sustainable Development Goals. Learn more at unaids.org and connect with us on Facebook, Twitter, Instagram and YouTube.
Press centre
Download the printable version (PDF)
Press Release
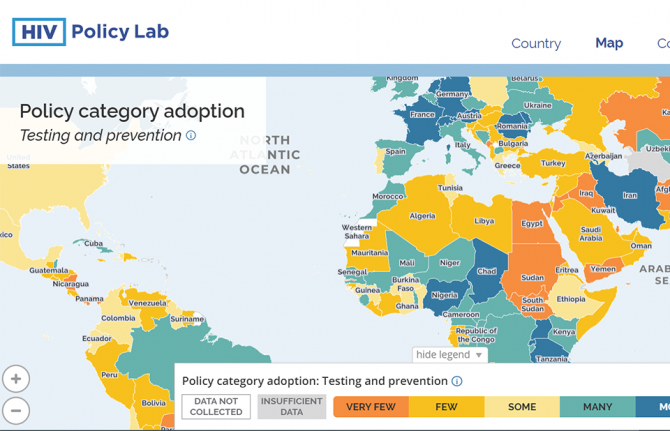
New HIV Policy Lab uses law and policy data in the HIV response
29 September 2020 29 September 2020WASHINGTON, D.C./GENEVA, 29 September 2020—Despite decades of scientific advance in the HIV response, progress remains uneven, with some countries rapidly reducing AIDS-related deaths and new HIV infections and others seeing increasing epidemics. Laws and policies are driving a significant part of that divergence.
Launched today, the HIV Policy Lab is a unique initiative to gather and monitor HIV-related laws and policies around the world.
“Laws and policies are life or death issues when it comes to HIV. They can ensure access to the best that science has to offer and help people to realize their rights and live well, or they can be barriers to people’s well-being. Like anything that matters, we need to measure the policy environment and work to transform it as a key part of the AIDS response,” said Winnie Byanyima, UNAIDS Executive Director.
The HIV Policy Lab is a data visualization and comparison tool that tracks national policy across 33 different indicators in 194 countries around the world, giving a measure of the policy environment. The goal is to improve transparency, the ability to understand and use the information easily and the ability to compare countries, supporting governments to learn from their neighbours, civil society to increase accountability and researchers to study the impact of laws and policies on the HIV pandemic.
According to Matthew Kavanagh, Director of the Global Health Policy & Politics Initiative at Georgetown University’s O’Neill Institute, “Policy is how governments take science to scale. If we want to improve how policy is used to improve health outcomes, it is essential to monitor and evaluate the policies that comprise it.”
“Reducing stigma and making care easier to access are fundamental for improving the lives of people living with HIV—and those are all consequences of policy choices. Tracking these choices is a key tool for improving them, and ensuring justice and equity for people living with HIV,” said Rico Gustav, Executive Director of the Global Network of People Living with HIV.
The HIV Policy Lab draws information from the National Commitments and Policy Instrument, legal documents, government reports and independent analyses to create data sets that can be compared across countries and across issues. The goal of the HIV Policy Lab is to help identify and address the gaps between evidence and policy and to build accountability for a more inclusive, effective, rights-based and science-based HIV policy response.
The HIV Policy Lab is a collaboration between Georgetown University and the O’Neill Institute for National and Global Health Law, UNAIDS, the Global Network of People Living with HIV and Talus Analytics.
About the Georgetown University O’Neill Institute for National and Global Health Law
The O’Neill Institute, housed at Georgetown University, was established to create innovative solutions to the most pressing national and international health concerns, with the essential vision that the law has been, and will remain, a fundamental tool for solving critical health problems. The Georgetown University Department of International Health is home to scholarship in public health, economics, political science, and medicine. Georgetown’s Global Health Initiative serves as a university-wide platform for developing concrete solutions to the health challenges facing families and communities throughout the world. Read more at oneillinstitute.org and connect with us on Twitter and Facebook.
About UNAIDS
The Joint United Nations Programme on HIV/AIDS (UNAIDS) leads and inspires the world to achieve its shared vision of zero new HIV infections, zero discrimination and zero AIDS-related deaths. UNAIDS unites the efforts of 11 UN organizations—UNHCR, UNICEF, WFP, UNDP, UNFPA, UNODC, UN Women, ILO, UNESCO, WHO and the World Bank—and works closely with global and national partners towards ending the AIDS epidemic by 2030 as part of the Sustainable Development Goals. Learn more at unaids.org and connect with us on Facebook, Twitter, Instagram and YouTube.
About GNP+
GNP+ is the global network for and by people living with HIV. GNP+ works to improve the quality of life of all people living with HIV. GNP+ advocates for, and supports fair and equal access to treatment, care and support services for people living with HIV around the world. Learn more at gnpplus.net and connect with GNP+ on Facebook, Twitter and Instagram.
Contact
O’Neill InstituteLauren Dueck
Lauren.Dueck@Georgetown.edu
UNAIDS
Sophie Barton-Knott
bartonknotts@unaids.org
GNP+
Lesego Tlhwale
ltlhwale@gnpplus.net
Press centre
Download the printable version (PDF)

Feature Story
Five UNAIDS country directors taking the lead in the COVID-19 response
11 June 2020
11 June 2020 11 June 2020The experience of the UNAIDS Country Director for El Salvador, Celina Miranda, a trained medical doctor, has been very useful during the COVID-19 outbreak. When the United Nations Resident Coordinator nominated her to be the COVID-19 response team leader within the United Nations in the country, she was honoured.
“I accepted the challenge, since the experience of working at UNAIDS on HIV has given me the skills needed to handle these types of situations,” she said.
To date, she has handled six confirmed COVID-19 cases of United Nations personnel from different agencies. “Some went to hospital, while others self-quarantined, and all are already emerging from the acute stage,” Ms Miranda said.
A main task for COVID-19 coordinators is to determine whether local hospitals could admit and treat United Nations personnel and their dependents. El Salvador was not ready for the pandemic, she said, which added to the pressure.
Ms Miranda, along with four other UNAIDS country directors, has been nominated by the United Nations Country Teams as COVID-19 coordinators in their respective countries.
Vladanka Andreeva in Cambodia, Yafflo Ouattara in Chad, Job Sagbohan in Burkina Faso and Medhin Tsehaiu in Kenya have all felt honoured to take on such a responsibility.
Ms Andreeva explained how in early March the United Nations in Cambodia set up a United Nations Internal COVID-19 Preparedness and Response Team, and she was asked to lead the efforts in ensuring that more than 2500 United Nations staff and their dependents have access to the latest COVID-19 information, treatment, care and support. She developed a contingency plan for the United Nations family and supported the establishment of a medical evacuations process and mental health support services for staff.
Mr Sagbohan, a trained medical epidemiologist who has worked for the World Health Organization during Ebola and yellow fever outbreaks, said he spent a lot of time reassuring employees in order to overcome stress and fear. “Staff were scared, so during the lockdown period I got up to 300 calls a week despite the regular virtual town hall briefings for staff across Burkina Faso.”
He explained that despite UNAIDS’ size and lack of resources compared to other agencies, knowing about infectious diseases has helped greatly. He quickly requested focal points from different organizations and set up a United Nations taskforce against COVID-19. “I have been able to tap into a solid group of motivated people to help me and it has made all the difference.”
For Yafflo Ouattara, the COVID-19 coordinator role suits UNAIDS country directors perfectly. “We are used to getting buy-in from our Cosponsors, so joint teamwork is part of our DNA,” he said. His main task in Chad has been expanding intensive care units and setting up a strong referral system for the management of severe cases. Nearly 7000 United Nations employees and dependents are spread out across the country, some in places where there is no overnight care.
Like others, he also helped out with the national COVID-19 contingency plan to ensure that people living with HIV have access to treatment and care.
He said that the pandemic highlighted gaping holes in the country’s health system. “Not only were key investments in intensive care never made, some of the basics, like gloves, masks, soap, have been missing all along.”
Living in a COVID-19 world means a lot of readjustments. “We have an opportunity to step in and make our voices heard to overhaul systems,” Mr Ouattara said.
Medhin Tsehaiu agrees. She has been proud to see UNAIDS be part of the greater discussion.
“We are present and we are very actively and willingly doing our share,” she said. But she believes that COVID-19 has forever changed how people work.
All the virtual meetings and no travel has meant that people were much more available, so there was non-stop communication, but it was very time-consuming, she explained. “The crisis brought us together, whether we like it or not, and that has required a lot of collaboration,” Ms Tsehaiu said.
Aside from her long list of tasks as a COVID-19 coordinator, she and a few others started the United Nations Kenya solidarity fund. After much back and forth, they opened a bank account where staff can choose to contribute money during a three-month period that will be dispatched to people in need.
“It’s a way for employees to show empathy and support to the Kenyan people during these difficult times,” she said.
Speaking of solidarity, Ms Andreeva said that the pandemic really tested United Nations reform at the country level, not just in terms of responding to the pandemic but also regarding duty-of-care issues. According to a survey in May, 90% of the staff in Cambodia said that the United Nations leadership at the country level is making the right decisions managing the crisis.
During a virtual town hall meeting of 300 United Nations staff members in El Salvador recently, there was also positive feedback. Ms Miranda said she doesn’t ask for accolades or additional thanks. “I just enjoy helping people and seeing them recover, living their lives fully.”
Our work
Related
Documents
Report of the UN Secretary-General on the Implementation of the Declaration of Commitment on HIV/AIDS and the political declarations on HIV/AIDS (Seventy-fourth session of the General Assembly) 1 April 2020 - A/74/778
01 April 2020
This is a milestone year for the global AIDS response. The end of 2020 marks the deadline for targets agreed in 2016 by the General Assembly, in its resolution 70/266, to front-load investment, accelerate the response and end the epidemic by 2030.
Related
 Global leaders commit to accelerating global efforts to end AIDS as a public health threat by 2030
Global leaders commit to accelerating global efforts to end AIDS as a public health threat by 2030
13 December 2024

 Upholding dignity for everyone: Ariadne Ribeiro Ferreira
Upholding dignity for everyone: Ariadne Ribeiro Ferreira
21 November 2024
 Evelyn Siula: A journey of strength and solidarity
Evelyn Siula: A journey of strength and solidarity
18 November 2024

 The AIDS response is recognized as a beacon of hope and guide for revitalizing multilateralism at the 79th UN General Assembly
The AIDS response is recognized as a beacon of hope and guide for revitalizing multilateralism at the 79th UN General Assembly
27 September 2024
 Leaders pledge bold action to end AIDS by 2030
Leaders pledge bold action to end AIDS by 2030
24 September 2024


Feature Story
Modelling the extreme—COVID-19 and AIDS-related deaths
25 May 2020
25 May 2020 25 May 2020Kimberly Marsh, a senior adviser on modelling and epidemiology, has worked for UNAIDS for six years. She supports countries in estimating the impact of the HIV epidemic globally and regionally.
Can you tell me more about the latest modelling report that you are a co-author of, which examines the potential for HIV service disruption in times of COVID-19 in sub-Saharan Africa?
This work looks at potential disruptions in sub-Saharan Africa owing to the COVID-19 pandemic on HIV services that might have an impact on HIV incidence—the number of new HIV infections—and on the number of AIDS-related deaths in excess to those we might have observed if we hadn’t had the COVID-19 pandemic.
We are particularly interested in those question because we know that more than two thirds of all people living with HIV worldwide are living in sub-Saharan Africa. That’s 25.7 million people living with HIV, 1.1 million new HIV infections and around 470 000 deaths from AIDS-related causes in 2018. Among all people living with HIV in the region, 64% of people are on life-saving antiretroviral therapy, which also prevents further new HIV infections.
It is really important that we’re able to ensure they will have access to services. In the models, we looked at service disruptions—a complete disruption of any HIV-related services over a three-month and a six-month period of time. And we looked at the impact after one year and five years. Now remember, these are just scenarios, and extreme ones. We don’t expect this to happen, but it helps us to answer two questions: what HIV-related services are most important to prevent additional deaths and new HIV infections and what might happen if we don’t mitigate or address those disruptions.
From this huge amount of work, what are the two key takeaways?
The modelling work predicted that with a six-month disruption in HIV treatment there could be an excess of 500 000 deaths in sub-Saharan Africa. So, when you look at UNAIDS estimates of AIDS-related deaths over time, that would take us back to about 2008, when we had nearly a million deaths.
There is no doubt about it, HIV treatment is critical. Ensuring that HIV treatment is available to people who need it during the three- to six-month periods is the most important thing that countries can do to prevent excess deaths and HIV incidence. All countries should work to ensure that supply chains are providing them with enough medicines to distribute and that people have sufficient medicines so that they can take them over the coming months.
The second thing to say is that these are projections and that there is still time to ensure that people get the HIV treatment services they need.
Let’s prevent what this model potentially predicts and let’s get HIV medicines to the people who are living with HIV.
What about HIV prevention? Does condom availability have an impact?
The models showed that when you look at prevention services, condom availability impacted the results. I think it is important to say that this is a treatment lesson primarily, but things like access to condoms is really important. We saw around a 20–30% relative increase in HIV incidence over one year if condoms were not available for six months. This is definitely something that we should be focusing on.
Can you tell us a little bit more about the impact on mother-to-child transmission of HIV in these scenarios?
In the scenarios, we looked at the potential for HIV testing services to be disrupted as well as for women to not get medicine to prevent transmission of HIV to their children. And what the various models found was that by removing those medicines—which have had an extremely important impact in terms of reducing new child HIV infections over the past five to 10 years—you could see rises in new child HIV infections in selected countries anywhere up to 162%. It really is critical to maintain prevention of mother-to-child transmission of HIV services.
You have said this was an extreme scenario, not a prophecy, but yet you still believe in modelling?
Models are very important for exploring questions that countries routinely pose to UNAIDS and the World Health Organization in terms of thinking of strategic approaches to responding to HIV in their countries. Models aren’t perfect, but they have a lot to tell us and I think in this instance it really highlights some of the strategies that will be important over the coming months as COVID-19 impacts or potentially impacts sub-Saharan Africa.
Related

Feature Story
Dealing with COVID-19 in Cameroon
11 May 2020
11 May 2020 11 May 2020Q&A with UNAIDS Country Director Savina Ammassari
Savina Ammassari has been the UNAIDS Country Director for Cameroon since 2018. Before that, she worked for UNAIDS in India, Myanmar and Cambodia as a Strategic Information Adviser. She has supported initiatives promoting sustainable development, equity and human rights in more than 20 countries.
Because she has lived and worked in so many countries and speaks many languages, she considers herself quick to adapt, but COVID-19 has definitely tested her.
Savina, did you feel like COVID-19 was a tsunami coming your way?
Yes, indeed, I saw the tsunami coming. I’d followed the COVID-19 outbreak in China, the rapidly unfolding epidemic in Italy, my home country, which already has claimed more than 24 000 lives. I was acutely aware that many countries in sub-Saharan Africa, including Cameroon, would be ill-prepared to address the devastating health and economic impacts of COVID-19, where fragile health systems and chronic poverty represent significant challenges for government, community and United Nations system responses to the pandemic.
The realities of the crisis enveloping the world were starkly brought home to me when my brother-in-law, working as a surgeon in Brescia, the epicentre of the Italian epidemic, developed severe COVID-19 symptoms, leading to bilateral pneumonia. Fortunately, he was ventilated and received experimental treatments. His life has been saved. But I know this will not be the case for everyone, especially in countries with weaker health-care systems.
Cameroon is now the COVID-19 epicentre in western and central Africa. The first cases were detected at the airport of the capital, Yaoundé. Additional cases were soon recorded in Douala, the largest city of the country. Despite early measures taken by the Government to isolate initial cases, testing and contact tracing, community transmission has taken hold. Limited access to testing services makes it difficult to know the extent of transmission.
The Cameroon response has faced significant constraints, not least the capacity to scale up testing and expand contact tracing and the provision of intensive care unit/ventilation support for the seriously ill, as well as adequate personal protective equipment for medical staff. The rapid implementation of community education programmes, emphasizing hand hygiene and social distancing, is an ongoing challenge, especially in poor, often overcrowded, urban areas.
How did Cameroon prepare? In Cameroon, there initially was a sense of optimism that, somehow, Africa, unlike other regions, would manage to avoid the catastrophic consequences of the pandemic. There was little awareness that Cameroon was most likely just a matter of a few weeks behind.
Today, Cameroon is the most affected country in the region and second in sub-Saharan Africa, with a quickly rising rate of infections. The scarcity of test kits obviously hides the real number of infections. Counting individual infections, recoveries and fatalities does not provide the real picture. UNAIDS advocated for a modelling of the epidemic in order to enable quantification of health-care needs and procurement.
As the first COVID-19 cases were detected in Yaoundé, a small number of health-sector officials gathered with the Minister of Health to discuss and plan epidemic containment and impact mitigation measures. I was one of the United Nations officials requested to be part of the group, given UNAIDS’ experience in epidemic management. I underscored the need to build on existing systems and make use of the community-driven efforts of the national AIDS response. I advocated for frontloading investments in communication and community mobilization to prevent COVID-19 infections, using a multisectoral approach.
The multisectoral response fell into place through the direct involvement of the United Nations Resident Coordinator (UNRC) with my support. I facilitated the UNRC’s efforts to connect the Minister of Health with development partners in weekly teleconference calls. Partners were ready to assist but lacked information on the most immediate needs.
UNAIDS has supported the Ministry of Health to model the COVID-19 epidemic to better understand and quantify needs. This has been done through teleconferencing, with the participation of various technical and financial partners. It has helped with the prioritization of needs and the quantification and costing of urgently required supplies and equipment. Partners were ready to support this effort, but required not only a modelled, costed national COVID-19 response plan but also a well-articulated procurement schedule based on the plan. UNAIDS has also successfully advocated for the establishment of a strategic information working group to analyse more in-depth data from surveillance, model the epidemic, and monitor and evaluate the COVID-19 response.
Communicating is indeed key. But how do you deal with things as basic as the lack of running water in many sub-Saharan African countries, making handwashing difficult. How are people coping with this and other measures, such as physical distancing?
This is indeed a major challenge in Cameroon as there is a lack of consistent water supply in many urban and rural communities. The use of hand sanitizers is not an affordable option for most people and locally produced product is not necessarily quality assured and safe for use.
Similarly, physical distancing and self-isolation are remote, often unrealistic options for communities where large numbers of people, as a rule, share common spaces in their home and community environments. The government has put in place a series of strict measures to contain the spread of COVID-19 (closing schools and educational or training institutions, banning gatherings of all kinds, imposing the use of face masks on public transport), although a comprehensive lockdown has not been promulgated to date. There are legitimate concerns on how a full lockdown could affect the majority of people, as more than 80% of the population work in the informal sector and live hand-to-mouth. Yet, from a public health perspective, lockdowns are a must. Balancing concerns is a major challenge.
Savina, you have never shied away from challenges. Would you say this is the biggest challenge you have faced, and why?
Yes, this crisis is unprecedented, unpredictable. I’m concerned at how the COVID-19 pandemic will affect not only our staff and their dependents but also people living with HIV, who need to continue accessing antiretroviral therapy and services, and people who are already stigmatized, vulnerable and socially and economically marginalized.
We have already witnessed a worrisome rise in stigma and discrimination against members of key populations in Cameroon and are making sure that the UNCT and partners keep human rights issues high on the agenda.
Our work is already challenging in normal times as Cameroon is facing enormous development and humanitarian hurdles. Already, Cameroon’s humanitarian crises on three fronts are not getting enough international attention. It’s the least funded humanitarian crisis worldwide. The COVID-19 epidemic multiplies these challenges several times over.
UNAIDS is mobilizing communities and networks in COVID-19 prevention work and making sure that civil society is adequately consulted and involved in the national response to the new virus.
How do you unwind in the evening? How do you recharge your batteries?
I’m afraid I don’t give enough time to relaxing, as I work around the clock, which isn’t good. Perhaps one of the challenges of COVID-19 is to take up new interests outside of work, that can be sustained and enjoyable well into the future.
What are the lessons learned? Will you do things differently from now on?
I’ve learned once again that unity makes force. In unpreceded emergencies like the current one, where no one has the answer or a magic bullet, everyone’s competence and experience is needed. Connecting people, bringing in resources, getting a transparent exchange—all this is paying off. It requires strong leadership and a cohesive team effort.
Our work
Region/country
Related
 Impact of the pause of US foreign assistance in Côte d'Ivoire
Impact of the pause of US foreign assistance in Côte d'Ivoire
19 February 2025

Feature Story
UNAIDS—a leading organization for gender equality
13 March 2020
13 March 2020 13 March 2020A report on the progress made over the past 12 months by organizations active in the health sector to implement policies that promote gender equality, non-discrimination and inclusion in the workplace has once again rated UNAIDS as a “very high scoring” organization.
UNAIDS is one of only 13 out of the top 200 global health bodies—funders, nongovernmental organizations, corporate organizations and others with a presence in at least three countries—to be designated as very high scoring. A further 27 organizations were “high scorers”.
“I’m proud that UNAIDS is seen as gender-responsive and inclusive,” said Winnie Byanyima, Executive Director of UNAIDS. “But we must continue to build on these results—we’ve still got a long way to go.”
Researchers assessed the gender and geography of global health leadership, and the availability of gender and diversity policies in the workplace. The report also assessed whether organizations address the crucial role of gender in their health investment programmes and the health priorities they address.
While identifying some progress towards gender equality across the 200 organizations surveyed, the report warns that the pace of change is too slow, estimating that it will take more than 50 years to reach parity at the senior levels of global health organizations.
“Many of the 200 organizations we reviewed are falling short on the equality measures that they purport to uphold. More than 70% of the chief executives and chairs of boards are men, while only 5% are women from low- and middle-income countries,” said Sarah Hawkes, co-founder of Global Health 50/50 and Professor of Global Public Health at University College London.
Power, privilege and priorities is the third Global Health 50/50 report. Previous Global Health 50/50 reports have also found UNAIDS to be a gender leader, being rated in the top nine out of 140 organizations in 2018 and in the top 14 out of almost 200 organizations in 2019.
Related



Feature Story
UN Cares: putting people first in Jamaica’s HIV response
02 December 2019
02 December 2019 02 December 2019Erva-Jean Stephens works as a Strategic Information Adviser in the UNAIDS Country Office in Jamaica. She describes her role as using evidence-informed data to shape programmes and policies that contribute to the country’s development.
Ms Stephen’s professional career is entwined with an activist’s desire to see better health outcomes for ordinary Jamaicans.
“I try to serve people first,” says Ms Stephens. “People reach out to me because I make myself accessible and I easily relate to their needs. I naturally build networks outside of the work environment that I think might be beneficial to the work we do.”
She supports the nongovernmental organization Eve for Life because she believes that young women and girls living with or affected by HIV are being left behind with regard to international funding and programmatic focus. Beyond providing technical support to help Eve for Life increase its funding, Ms Stevens has mobilized private sector organizations and UN Cares, the United Nations system-wide workplace programme on HIV, to raise funds and create care packages for young women and their children.
Under her leadership, UN Cares Jamaica has trained United Nations staff members in the country on issues such as unconscious bias and the human rights of lesbian, gay, bisexual, transgender and intersex people and of people who use drugs. In 2016, the United Nations team in Jamaica received an award from the United Nations Secretary-General for its work on raising awareness about HIV and noncommunicable diseases.
In 2018, UN Cares Jamaica launched UN Moves. This is an offshoot of a project led by the Ministry of Health that aims to harness the power of the private and public sectors to help create a healthier, happier population through nutrition, exercise and education. But for Ms Stevens, the most critical area of UN Cares’ work remains addressing HIV-related stigma and discrimination.
“There needs to be ongoing training on cultivating and maintaining a model work environment where stigma and discrimination have no place. Sometimes we may not realize to what extent people are looking at us in the United Nations and how important it is for us to walk the talk,” said Ms Stevens. She thinks about her own journey and how through the UN Cares programme she has learned to identify and uproot her own biases.
Ms Stevens has a degree in environmental health and food safety and a master’s degree in public health with a specialization in medical epidemiology. She began her career with the Ministry of Health, using monitoring and evaluation techniques to ensure outbreaks of malaria and food-borne illnesses were quickly brought under control.
She hopes to be part of the team that sees the end of the AIDS epidemic.
“When you look at the history of the Caribbean in terms of eradicating diseases, political commitment and community involvement have always intersected,” she explains. “To meet our commitments on controlling the transmission of HIV, we need to see more meaningful community engagement and leadership, supported by political will. I am here to provide the strategic information necessary to help realize that goal.”
Focus on
Region/country
Related
 U=U can help end HIV stigma and discrimination. Here’s how
U=U can help end HIV stigma and discrimination. Here’s how
27 February 2025
Comprehensive Update on HIV Programmes in the Dominican Republic
19 February 2025