Data

Update
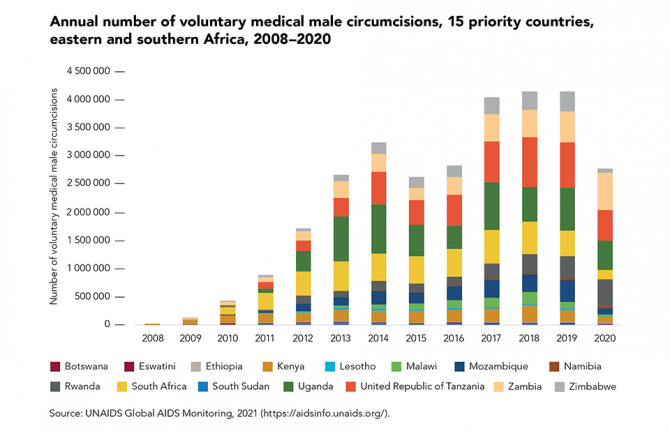
Male circumcisions disrupted by COVID-19, fall short of the 2020 target
29 November 2021
29 November 2021 29 November 2021In areas with high HIV prevalence and low rates of male circumcision, voluntary medical male circumcision (VMMC) can greatly contribute to HIV prevention. Despite this, there was a steep drop in the number of VMMCs performed in the 15 priority countries in 2020, due mainly to service disruptions caused by the COVID-19 pandemic: approximately 2.8 million procedures were performed in 2020, compared with 4.1 million in 2019.
Several countries suspended their programmes when the pandemic took hold, including South Africa. Despite this, programmes in some countries proved resilient enough to recover quickly and expand during the rest of 2020—notably in Rwanda and Zambia, where programme coverage grew by about 15%. In these countries, adjustments for the safe continuation of VMMC services during COVID-19 included changes in promotion and demand generation, client transportation, service delivery at a health facility or in the community and post-procedure follow-up appointments.
A total of about 18 million VMMCs were performed in 2016–2020, far shy of the 2020 target of 25 million. As well as COVID-19, an additional setback in 2015 and 2016 was the detection of tetanus cases in Uganda, which led to activities being scaled back in that country.
Our work



Documents
UNAIDS data 2021
29 November 2021
The 90–90–90 targets were missed, but not by much. At the end of 2020, 84% of people living with HIV knew their HIV status, 87% of people living with HIV who knew their HIV status were accessing antiretroviral therapy, and 90% of people on treatment were virally suppressed.




Update
Race affecting HIV service provision in the United States of America
15 November 2021
15 November 2021 15 November 2021HIV service disparities by race have been documented in several parts of the developed world.
In the United States of America, black people account for a disproportionately large percentage of new HIV infections in the country: 41% in 2019, although they represent only about 13% of the national population. This is in part due to lower coverage of HIV prevention services. Just 8% of black Americans and 14% of Hispanics/Latinos who were eligible for pre-exposure prophylaxis were prescribed it, compared to 63% of whites.
Studies also report significant racial disparities in HIV treatment outcomes, with delayed initiation of treatment and care, lower adherence to antiretroviral therapy, increased stigma and discrimination, mistrust of or lack of access to health-care providers and inadequate access to health insurance among the contributing factors. Many of these gaps are among black and Latino gay men and other men who have sex with men, who must contend with both racial inequalities and homophobia.
Related
 Government ensures continuity of treatment in Malawi
Government ensures continuity of treatment in Malawi
10 February 2025
, South Africa, 2010–2020")
Update
Retention in care a growing concern
08 November 2021
08 November 2021 08 November 2021Data from South Africa highlight the challenge faced by many treatment programmes when it comes to successfully retaining people in HIV care.
The HIV treatment programme in South Africa reaches more people living with HIV than any other in the world, with more than 5 million adults (aged 15 years and older) receiving antiretroviral therapy in 2020. Among the 2.5 million adults living with HIV in South Africa who are not on treatment, a steadily increasing percentage are people who had started treatment but are no longer receiving it.
Efforts to support people on treatment to maintain treatment and achieve durable viral suppression are critical to improving health outcomes, maximizing the preventive benefits of treatment and preventing the emergence of drug-resistant strains of HIV. The World Health Organization recently updated its HIV treatment guidelines with a new recommendation to trace people who have disengaged from care and provide support for re-engagement.

Update
Harm reduction services reduce new HIV infections
01 November 2021
01 November 2021 01 November 2021The neighbouring Baltic states of Estonia and Latvia offer starkly contrasting examples of how different public health approaches affect HIV epidemics among people who inject drugs. In the early 2000s, the two countries had among the highest rates of HIV diagnosis in Europe. As was the case for many European countries at that time, the sharing of non-sterile injecting equipment among drug users was fuelling their HIV epidemics.
The two epidemics began to diverge in the mid-2000s. According to the HERMETIC study, new HIV infections in Estonia declined by 61% countrywide and by 97% among men who inject drugs between 2007 and 2016.
Latvia’s HIV epidemic followed a different trajectory. The HERMETIC study highlights that, between 2007 and 2016, new HIV infections increased by 72% overall. By 2016, overall HIV incidence in Latvia was almost double that in Estonia (35 cases per 100 000 people versus 19 cases per 100 000).
Both epidemics centred largely on the sharing of injecting equipment by people who inject drugs, and probably on unprotected sex between people who inject drugs and their sexual partners. The HERMETIC study concludes that the main difference between the two epidemics lay in the availability of harm reduction services.
Needle–syringe programmes had been operating in Latvia since 1997, but on a very limited scale. As late as 2016, Latvia was distributing about 93 needle–syringes per drug user per year; neighbouring Estonia was distributing 230 per user per year. Both countries expanded access to opioid substitution therapy, which is proven to reduce drug injecting and HIV transmission, and improved HIV testing and antiretroviral therapy services for people who inject drugs. Although access to opioid substitution therapy remained limited in both countries, it was higher in Estonia than in Latvia.
The HERMETIC study’s results indicate that by 2016, about half the people who inject drugs in Estonia were taking HIV tests in a 12-month period—and three quarters of those who tested HIV-positive were on antiretroviral therapy. In Latvia, meanwhile, about 10% of people who inject drugs took an HIV test in any given year between 2007 and 2016, and only 27% of those living with HIV were on antiretroviral therapy. Slow adoption of international HIV treatment guidelines contributed to the low treatment coverage in Latvia.
Related
Government ensures continuity of treatment in Malawi
10 February 2025
Documents
The response to HIV in western and central Africa
29 October 2021
The HIV response across western and central Africa is improving, but not fast enough to end AIDS as a public health threat by 2030. Over the past year, the COVID-19 pandemic has disrupted HIV and other health services, and it has highlighted the vulnerability of people in the region to public health, climatic, socioeconomic and security shocks, along with the pressing need for inclusive social protection systems.
Related
 U=U can help end HIV stigma and discrimination. Here’s how
U=U can help end HIV stigma and discrimination. Here’s how
27 February 2025
Impact of the pause of US foreign assistance in Côte d'Ivoire
19 February 2025
Government mitigation measures in Cameroon
09 February 2025

Update
Financial shortfalls hold back the HIV response in western and central Africa
25 October 2021
25 October 2021 25 October 2021Underinvestment in the HIV responses of low- and middle-income countries was a major reason why the global targets for 2020 were missed. Financial resource availability during the past five years was consistently below the resources needed, and in 2020 it was 29% less than the US$ 26 billion target for that year (in constant 2016 US dollars).
In western and central Africa, large resource shortfalls and continued reliance on out-of-pocket expenditures (such as user fees for health services) are associated with more modest declines in the incidence of HIV infection and the rate of AIDS-related mortality compared to eastern and southern Africa, where a combination of domestic and international investments has fuelled the rapid expansion of HIV prevention, testing and treatment in areas with a high burden of HIV, resulting in strong and steady reductions in the rate of HIV infections and AIDS-related mortality.
Related
U=U can help end HIV stigma and discrimination. Here’s how
27 February 2025
Impact of the pause of US foreign assistance in Côte d'Ivoire
19 February 2025

Update
Upper-middle-income countries pay more for HIV medicines, but price reductions can be achieved
18 October 2021
18 October 2021 18 October 2021The cost of antiretroviral medicines has a major effect on resource needs for HIV responses. Currently, the average prices for first- and second-line antiretroviral therapy are broadly similar in low- and lower-middle-income countries, but are substantially higher in upper-middle-income countries.
For example, countries in eastern Europe and central Asia and in Latin America tend to pay considerably higher prices for antiretroviral medicines compared with countries in other regions. Further price reductions for antiretroviral medicines and other key HIV commodities can be achieved through the strategic use of flexibilities under the Agreement on Trade-Related Aspects of Intellectual Property Rights (TRIPS) and by rearranging procurement and supply management systems to take advantage of economies of scale. If these and other cost savings are made, a 17% increase in resources for HIV testing and treatment can result in a 35% increase in the number of people receiving treatment by 2025—enough to reach the 95–95–95 testing and treatment targets.
Our work
Related
U=U can help end HIV stigma and discrimination. Here’s how
27 February 2025
Documents
2021 Global AIDS Update Slideset
14 July 2021

Related
UNAIDS data 2024
02 December 2024
Slide deck - 2024 global AIDS update
22 July 2024
Core epidemiology slides
22 July 2024
 and adolescents (aged 10-19 years), global, 2000-2020. Source: UNAIDS epidemiological estimates, 2021")
Update
Slow progress on AIDS-related deaths among adolescents
04 October 2021
04 October 2021 04 October 2021Current inequalities in HIV testing and treatment for children living with HIV and trends in historical coverage of services to prevent vertical (mother-to-child) transmission of HIV are driving year-on-year trends in AIDS-related mortality.
Reductions in AIDS-related deaths among children and adolescents are steepest among children aged 0 to 9 years (a 60% decline since 2010), reflecting both improvement in efforts to prevent new vertical infections and efforts to diagnose and treat children in the months following childbirth and during breastfeeding.
However, among adolescents (aged 10–19 years), progress is slower, with AIDS-related deaths declining just 37% over the same period.
The single biggest paediatric treatment challenge is to rapidly find children living with HIV who were missed at birth or during breastfeeding and link them to care. Scale-up of rights-based index, family and household testing and self-testing, and integrating HIV screening with other child health services, can help close this gap.
Our work
Related
U=U can help end HIV stigma and discrimination. Here’s how
27 February 2025