Internally displaced persons IDP
unaids.org
UNAIDS




Feature Story
Africa’s welcome mat: stories of hope and resilience from refugees in Uganda
29 March 2018
29 March 2018 29 March 2018“Right now, I just want to go to a country where there is peace,” says a young student who fled the ...
“Right now, I just want to go to a country where there is peace,” says a young student who fled the conflict in his home country, the Democratic Republic of the Congo. His new home is Kyangwali Refugee Settlement Area in the Hoima District of Uganda—the place that will give him a chance to fulfil his dream of a peaceful life.
The Kyangwali Refugee Settlement Area lies on the banks of Lake Albert on the border between southern Democratic Republic of the Congo and northern Uganda. Most of the refugees in Kyangwali are fleeing interethnic conflict in eastern Democratic Republic of the Congo and making the perilous journey into Uganda on fishing boats across Lake Albert. Since January 2018, approximately 59 000 people have made the crossing. On a normal day 500 refugees arrive; on a busy day it can be as many as 2000.
Families arrive with whatever personal belongings they can carry—from mattresses and cookware to valuables, such as solar panels, piled high among the passengers in the boats. The boat ride can take as little as six hours if people travel in a motorized vessel or as much as 12 hours if they travel by canoe. “Boats sometimes run out of fuel in the middle of the lake and Ugandan marine police have to bail them out,” says Bornwell Kantande, Representative of the Office of the United Nations High Commissioner for Refugees in Uganda. “Other boats have capsized from overloading—at the peak of the influx of refugees as many as 200 people would pile onto a single canoe.”
Upon arrival at the Kyangwali reception centre, refugees are registered by aid workers and given a wristband for identification purposes. They receive high-energy biscuits and water and those who need it are given emergency health care. Refugees stay at the reception centre for a day or two before being transported to the settlement area, where they are allocated a small plot of land and material and equipment to build temporary shelter while they establish themselves.
In a recent visit to the reception centre, Michel Sidibé, UNAIDS Executive Director, witnessed first-hand the health services that are offered to newly arrived refugees at its small makeshift clinic. Here refugees obtain access to emergency health care and are informed about the minimum initial service package for reproductive health, which they receive throughout the different phases of new arrival: border crossing; the short stay at the reception centre; before transportation to the settlement area; and during settlement. Services include HIV testing and tuberculosis screening, prevention of mother-to-child transmission of HIV services, provision of HIV and tuberculosis treatment to people already on it and other sexual and reproductive health services.
During his visit, Mr Sidibé listened to the stories of many refugees, who told him not only of the impact that dislocation has had on their health and their lives, but also of their aspirations and dreams to make a better life for themselves and their families. “I heard stories of sadness, but also of hope and resilience,” says Mr Sidibé.
Uganda is home to the largest refugee population in Africa, with a population of almost 1.4 million refugees in 13 refugee settlements across the country. The majority of refugees are from South Sudan and the Democratic Republic of the Congo, the latter of which has close to five million displaced people—almost as many as in the Syrian Arab Republic.
“It is beyond admirable to selflessly offer refuge to hundreds of thousands of women, children and men who are in need of international protection,” remarked Mr Sidibé. “Uganda’s refugee policy is among the most progressive in the world and is a model for other countries to emulate.”
Region/country
Related
unaids.org
UNAIDS

Update
Time to act in South Sudan
09 February 2018
09 February 2018 09 February 2018A United Nations interagency task team has called for partners, donors, national authorities and oth...
A United Nations interagency task team has called for partners, donors, national authorities and others to act in South Sudan.
South Sudan has been ripped apart by civil war for the past two years. Tens of thousands of people have been killed and many others have fled their homes. Widespread reports have detailed looting, rape, enslavement and the use of children in armed conflict.
Two million people are internally displaced in the country and more than 1.95 million people have migrated to neighbouring countries. Food has become scarce and famine has followed.
The task team gives 16 recommendations in a new report, Time to act! Conflict, displacement, famine and the HIV response. Among these are that when targeting food assistance, people living with chronic illnesses, including HIV, should be included, in order to help them to adhere to their treatment. The report also urges the continuing distribution of medicines to treat HIV, sexually transmitted infections and tuberculosis and for condoms to be available through the country and in neighbouring countries.
South Sudan is one of the 38 countries that account for 90% of all new infections, and only 10% of people living with HIV in the country are on life-saving antiretroviral therapy. The conflict has weakened HIV services and host countries often cannot provide for the influx of refugees.
Related documents
Region/country
Related
unaids.org
UNAIDS

Sophie Barton-Knott
tel. +41 22 791 1697
bartonknotts@unaids.org
IOM
Jorge Galindo
tel. +41 22 717 9205
jgalindo@iom.int
Press Release
UNAIDS and IOM renew partnership agreement to promote access to HIV services for migrants and crisis-affected populations
08 December 2017 08 December 2017GENEVA, 8 December 2017—UNAIDS and the International Organization for Migration (IOM) today signed a...
GENEVA, 8 December 2017—UNAIDS and the International Organization for Migration (IOM) today signed a new cooperation agreement to promote access to HIV prevention, treatment, care and support services for migrants, mobile populations and people affected by humanitarian emergencies.
“Migrants and people displaced through conflict or emergencies must be supported and enabled through their journeys to exercise their right to health,” said Michel Sidibé, Executive Director of UNAIDS. “This new partnership agreement between UNAIDS and the International Organization for Migration will be essential in strengthening our efforts to make sure that no one is left behind.”
Under the new agreement, UNAIDS and IOM will encourage states to take steps to ensure access to HIV prevention, treatment, care and support and to reduce stigma, discrimination and violence. States will also be encouraged to review policies related to restrictions on entry based on HIV status, with a view to eliminating such restrictions.
“Migrants and mobile populations are exposed to a unique set of factors that render them more vulnerable to HIV, including limited access to health services and information as well as exposure to environments that are conducive to engaging in higher-risk behaviours,” said IOM Director General William Lacy Swing. “In order to achieve the Sustainable Development Goals and to meet the universal health coverage targets set therein, it is crucial that the rights of migrants to health be realized and effected through evidence-based, whole-of-government and cross-sector approaches, and the International Organization for Migration will continue to work closely with UNAIDS and other actors in jointly addressing these issues,” added Mr Swing.
IOM and UNAIDS will work to ensure a package of care for people living with HIV and/or tuberculosis in humanitarian emergencies and conflict settings to reduce their vulnerability to HIV, reduce the risk of treatment interruption and ensure access to quality healthcare and nutritious food.
UNAIDS and IOM will also tackle the multiple forms of discrimination against refugee and migrant women and girls and promote access to tailored comprehensive HIV prevention services for women and adolescent girls, migrants and key populations.
IOM and UNAIDS have a long-standing partnership. IOM is part of the United Nations joint teams on HIV at the country level and its HIV and population mobility programme complements the work of UNAIDS globally.
During the 108th session of the IOM Council, UNAIDS was granted observer status by IOM, a sign of strengthened cooperation between the two institutions.
UNAIDS
The Joint United Nations Programme on HIV/AIDS (UNAIDS) leads and inspires the world to achieve its shared vision of zero new HIV infections, zero discrimination and zero AIDS-related deaths. UNAIDS unites the efforts of 11 UN organizations—UNHCR, UNICEF, WFP, UNDP, UNFPA, UNODC, UN Women, ILO, UNESCO, WHO and the World Bank—and works closely with global and national partners towards ending the AIDS epidemic by 2030 as part of the Sustainable Development Goals. Learn more at unaids.org and connect with us on Facebook, Twitter, Instagram and YouTube.
IOM
Established in 1951, IOM is the leading inter-governmental organization in the field of migration and works closely with governmental, intergovernmental and non-governmental partners. With 169 member states, a further 9 states holding observer status and offices in over 100 countries, IOM is dedicated to promoting humane and orderly migration for the benefit of all. It does so by providing services and advice to governments and migrants.
Contact
UNAIDSSophie Barton-Knott
tel. +41 22 791 1697
bartonknotts@unaids.org
IOM
Jorge Galindo
tel. +41 22 717 9205
jgalindo@iom.int
Press centre
Download the printable version (PDF)
unaids.org
UNAIDS



Update
UNAIDS assisting the survivors of the floods in Sierra Leone
23 August 2017
23 August 2017 23 August 2017On 14 August, heavy rains, a mudslide and flash floods destroyed hundreds of homes and left many dea...
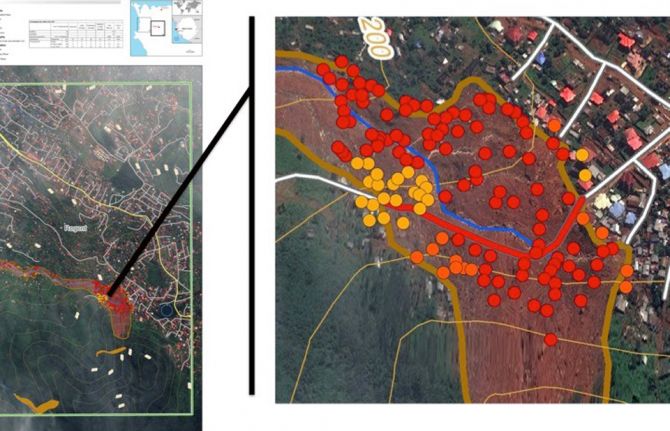
On 14 August, heavy rains, a mudslide and flash floods destroyed hundreds of homes and left many dead, injured or missing in Sierra Leone. In all, more than 500 houses were buried and destroyed and some 6000 people were severely affected. So far, more than 500 bodies have been recovered, with the number expected to rise. A mass burial for 300 people brought the country together and hardened the commitment to collectively recover from the tragedy.
An estimated 200 people living with HIV and their families were affected, with around 54 among the dead. Relief and rescue efforts by community members and first responders immediately began providing life-saving support.
People living with HIV and people at higher risk of HIV infection often become more vulnerable in times of emergency, owing to a lack of prioritization of their needs, lack of prevention services and disruption of treatment. In addition, people living with HIV, especially with weakened immune systems, are at higher risk of contracting malaria and waterborne diseases.
In the immediate aftermath of the disaster, UNAIDS’ priority has been to ensure the continuation and scale-up of antiretroviral therapy services, provide technical support to the Network of HIV Positives in Sierra Leone (NETHIPS), generate strategic information for fundraising and facilitate access for people living with HIV to food and non-food resources. UNAIDS has been participating in the broader disaster coordination structure within the United Nations and is supporting NETHIPS in the registration of people living with HIV affected by the disaster and in finding out their immediate needs.
In the medium and long term, UNAIDS, in collaboration with the United Nations interagency team, the National HIV/AIDS Secretariat, NETHIPS and the wider national disaster response coordination unit, will ensure that people living with HIV have access to support that includes the restoration of livelihoods, shelter construction and psychosocial services.
This crisis has put into sharp focus the fragility of Sierra Leone’s post-Ebola social safety nets. It is critical that the resources required for the response to HIV be included in the emergency fundraising appeals and that the country’s HIV catch-up plan be financed and implemented effectively.
Quotes
“Entire communities have been wiped out by the disaster. We need urgent support now.”
“Humanitarian crises exacerbate the HIV epidemic—vulnerabilities are increased, services are disrupted, people are uprooted and access to HIV prevention and treatment affected, leading to new HIV infections.”
Region/country
Related
 Impact of the pause of US foreign assistance in Côte d'Ivoire
Impact of the pause of US foreign assistance in Côte d'Ivoire
19 February 2025


unaids.org
UNAIDS



Conflict has forced more than a quarter of the population of South Sudan to flee their homes, disrupted crop production and destroyed livestock.
On 20 February 2017, famine was declared, which is already affecting 100 000 people, with a further 1 million people on the verge of famine
According to the United Nations Office for the Coordination of Humanitarian Affairs, some 1.9 million people have become internally displaced and another 1.6 million people have crossed the borders as refugees.
Feature Story
The incredible resilience of the people of South Sudan
30 March 2017
30 March 2017 30 March 2017Conflict has forced more than a quarter of the population of South Sudan to flee their homes, disrup...
Conflict has forced more than a quarter of the population of South Sudan to flee their homes, disrupted crop production and destroyed livestock. On 20 February 2017, famine was declared, which is already affecting 100 000 people, with a further 1 million people on the verge of famine. According to the United Nations Office for the Coordination of Humanitarian Affairs, some 1.9 million people have become internally displaced and another 1.6 million people have crossed the borders as refugees.
One of the regions most affected by the crisis is Equatoria, which is also the region with the highest burden of HIV in South Sudan. Around 90% of the 20 000 people on antiretroviral therapy in South Sudan live in Equatoria, where conflict and food insecurity are pushing people across the border to Uganda and the Democratic Republic of the Congo in their thousands daily, and out of reach of essential health services.
Many people living with HIV are among the refugees. Even when medicine is available, food insecurity is affecting their ability to take it regularly, as humanitarian agencies are struggling to meet the needs of hundreds of thousands of people with very little funding.
The resilience of people living with HIV affected by the crisis is incredible, even in the most difficult of situations. John* is a refugee in a camp near Ajumani in Uganda and a member of the South Sudan Network of People Living with HIV.
“A number of us were running out of antiretroviral medicines, and where we are settled there are no health facilities providing HIV treatment,” said John. “So we put together the little money we had and sent one of us back to Nimule in South Sudan to collect medicines for all of us. Luckily the doctor allowed and we now have some medicines, but when they finish, what do we do?”
Whether displaced or not, the main problem facing people living with HIV in South Sudan is food insecurity. People in towns and cities are also affected, with the majority of vulnerable families only eating one meal a day, and some going without food for days.
Stigma and discrimination is making the situation even more acute, as women living with HIV are often abandoned and left destitute because of their HIV status. Jane, a young mother of three living with HIV in Juba, the capital of South Sudan, found out her HIV status when she was pregnant with her third baby. Her husband and family abandoned her and her children, two of whom are also living with HIV. Jane does not have full-time employment and is struggling for her and her children to have just one meal a day.
“These days we have to insist on one pill a day, as we only eat once a day, if we get food that day, and we cannot take these medicines on an empty stomach. Others have stopped taking the medicines because they have no food,” she said.
Despite facing numerous challenges in her life, Jane volunteers as a “mentor mother” to support prevention of mother-to-child transmission of HIV services. She says of her work, “I like doing this, because we are many out there, but we fear discrimination if we disclose our HIV status. But with counselling, some of us are disclosing our status.”
In the 2016 United Nations Political Declaration on Ending AIDS, Member States committed to pursuing the continuity of HIV prevention, treatment, care and support and to providing a package of care for people living with HIV, tuberculosis and/or malaria in humanitarian emergencies and conflict settings, as displaced people and people affected by humanitarian emergencies face multiple challenges, including heightened HIV vulnerability, risk of treatment interruption and limited access to quality health care and nutritious food. UNAIDS is working with countries to ensure that the commitment is met.
* Names have been changed.
Resources
Region/country
Related
Documents
Progress report on the implementation of United Nations Security Council Resolution 1983
01 November 2016
The contribution of United Nations peacekeeping operations to the AIDS responses in a multitude of conflict and post-conflict situations to date underscores the importance of continued engagement by United Nations peacekeeping operations and other United Nations entities as the world endeavours to reach the level of service coverage required to end AIDS as a public health threat by 2030. Progress towards this ambitious goal requires a continuation of what is working well and addressing areas of inconsistency and inefficiency using the latest tools and knowledge on effective HIV responses.
Related
 Resilience amid crisis: strengthening the HIV response for displaced communities in Ethiopia
Resilience amid crisis: strengthening the HIV response for displaced communities in Ethiopia
02 December 2024
Take the rights path to end AIDS — World AIDS Day report 2024
26 November 2024

 Peru approves groundbreaking law to extend health coverage for migrants with HIV and TB
Peru approves groundbreaking law to extend health coverage for migrants with HIV and TB
21 October 2024
 Working to end gender-based violence in fragile settings
Working to end gender-based violence in fragile settings
28 August 2024
The missing link: Rethinking and reprioritizing HIV and gender-based violence in fragile settings
21 July 2024



unaids.org
UNAIDS

Suna Balkan, Head of the HIV/AIDS Working Group, Médecins Sans Frontières; Leo Zekeng, Deputy Director, UNAIDS Regional Support Team for Western and Central Africa; Bahya Mohamed, Executive Secretary, Interministerial Technical Committee on AIDS, Malaria and TB, Djibouti; Moses K. Jeuronlon, Adviser for HIV, Tuberculosis and Malaria. Harare, Zimbabwe, 30 November 2015. Credit: UNAIDS
Update
AIDS in emergency, conflict and humanitarian contexts
02 December 2015
02 December 2015 02 December 2015Emergencies and conflicts around the world are causing a dramatic growth in the number of refugees, ...
Emergencies and conflicts around the world are causing a dramatic growth in the number of refugees, asylum seekers and displaced people. Climate change and population growth also force people to migrate, thus adding to the numbers of people on the move.
In 2013, 314 million people were affected by emergencies, of which 67 million people were displaced by natural disasters and conflicts. Of these, 1.6 million were people living with HIV. Migration and displacement are major issues affecting people’s health, including reducing their access to HIV prevention, treatment, care and support services.
In order to assess the implications of such human displacements, UNAIDS organized an event at the 18th International Conference on AIDS and STIs in Africa, which is being held in Harare, Zimbabwe. The event provided an opportunity for key stakeholders to share experiences and best practices in order to ensure that people affected by humanitarian emergencies can continue to access life-saving HIV services.
Increased vulnerability to HIV because of sexual violence, sexual coercion and other human rights violations in humanitarian emergencies, conflict and post-conflict settings was also discussed at the event.
Quotes
“Around the world, 1.6 million people living with HIV have been displaced by natural disasters and conflict. Unless we deal appropriately with people in humanitarian emergencies, we are definitely not going to achieve the three zeroes. HIV must be integrated into national disaster preparedness and response plans.”
“Djibouti has initiated programming to help refugees, but we cannot do it alone. We would welcome the development and implementation of a regional plan with technical support for joint action and implementation so that we can work under a harmonized approach with other countries.”
“In areas prone to conflict, we need to be prepared in advance. Antiretroviral medicines, commodities, task-shifting plans and the involvement of communities must all be part of contingency planning. Preparation must also include extra long-term supplies of medicines and we have to be ready.”
“When Ebola hit Liberia, the entire health system was brought to a standstill. The impact was not only on the health system but on all aspects of the country as a whole. What we really need is a rapid response and availability of resources. Secondly, we need strong community engagement. When the health system broke down, we turned to the community.”
Region/country
Related

unaids.org
UNAIDS












Left to right: Martin Bloem, Senior Policy Advisor, Nutrition and HIV/AIDS Policy, World Food Programme; Paul Spiegel, Deputy Director, Public Health and HIV Section, Division of Program Support and Management UNHCR; Keynote speaker Noé Sebisaba of Burundi; Luiz Loures, Deputy Executive Director, UNAIDS.
Foreground: moderator Tom Ellman, Director, MSF Southern Africa Medical Unit (SAMU); background: "Towards ending AIDS by 2030: A conversation on the need for increased focus on HIV in emergency contexts" panelist George Okoth-Obbo, Assistant High Commissioner for Operations, UNHCR
"Towards ending AIDS by 2030: A conversation on the need for increased focus on HIV in emergency contexts" panelists Lt Gen Luiz G Paul Cruz, Director, Peacekeeping Strategic Partnership, DPKO; HRH Princess Sarah Zeid, Convener of the Humanitarian Settings work stream, Every Women Every Child.
"Enabling continued services for conflict-affected communities" panelists Marguerite Samba Maliavo, Minister of Health of the Central African Republic and Annie Clarisse Gonedet, Groupe de Soutien du Complexe Pédiatrique, Central African Republic.
"Delivering community services in public health emergencies" panelist Foday Sawi Lahai, Deputy Minister of Health and Sanitation, Sierra Leone
"Delivering community services in public health emergencies" panelist Alexandra Calmy, MSF field worker from the Ebola response
"Enabling protective environments for key populations" panelist Kassim Issack Osman, Minister of Health, Djibouti
"Enabling protective environments for key populations" panelist Gloria Fagade, YWCA Nigeria
"Enabling protective environments for key populations" panelist Sergii Dmytriiev, All-Ukrainian Network of People Living with HIV, Ukraine
"Enabling protective environments for key populations" panelist Manisha Dhakal, Executive Director, Blue Diamond Society Nepal
"Promoting preparedness and resilience" panelist Manuel Carballo, Executive Director, International Centre for Migration, Health and Development
"Promoting preparedness and resilience" panelist Karine Duverger, Health through Walls, Haiti
"Promoting preparedness and resilience" panelist Berna Beyrouthy, Lebanese Red Cross
Feature Story
Promoting greater focus on HIV in humanitarian emergencies
06 July 2015
06 July 2015 06 July 2015AIDS strategies and efforts must give greater priority to humanitarian emergencies and the millions ...
AIDS strategies and efforts must give greater priority to humanitarian emergencies and the millions of people affected by them, members of the UNAIDS governing body agreed at the thematic segment of the 36th meeting of the UNAIDS Programme Coordinating Board (PCB), which took place in Geneva, Switzerland, on 2 July.
New data presented at the thematic session by the Office of the United Nations High Commissioner for Refugees (UNHCR), the World Food Programme (WFP) and UNAIDS Secretariat estimate that of the 314 million people affected by humanitarian emergencies in 2013, 1.6 million people--or 1 in 22-- are living with HIV, and many thousands more are at risk.
“We are talking about incredible numbers of people and multiple layers of vulnerability. This is too big a scale and impact to ignore. We have to ensure that HIV prevention and treatment services are systematically integrated into emergency responses,” said Mr Michel Sidibé, Executive Director of UNAIDS.
The thematic session contemplated the vast and complex issue of HIV in emergency contexts, including the delivery of health and HIV services in the context of conflict situations, natural disasters, public health emergencies, displacement and migration. On protection issues, vulnerability to HIV due to sexual violence, human rights violations, restrictions, punitive laws and policies were topics of discussion. On resilience, participants talked about the need for community building and preparedness.
Panelists from a wide range of countries including Burundi, Central African Republic, Djibouti, Haiti, Lebanon, Liberia, Nepal, Nigeria, Sierra Leone and Ukraine told of the realities on the ground. They spoke of barriers and opportunities and gave examples of successful government and civil society efforts to address HIV in the wide variety of humanitarian emergency contexts.
In his keynote speech, former refugee Mr Noé Seisaba from Burundi, who founded the Stop SIDA organization that brings key HIV initiatives to refugee camps and settings, called for the community of people living with HIV to be involved in all aspects of planning and implementation. “I faced a lot of discrimination, but I broke my silence on HIV to try to make working on HIV a community issue and to show that we can intervene as refugees because we have a true understanding of the challenges and realities,” he said. “I am happy to see we are all talking about this issue, but I want to see concrete action.”
Many participants echoed that community involvement and empowerment of people living with and most affected by HIV are critical to achieve results for people in such difficult contexts. “If we are going to end the AIDS epidemic by 2030, we have to shine light on root causes of vulnerability in humanitarian settings and increase action to promote respect for rights and basic humanitarian dignity,” said Mr George Okoth-Obbo, Assistant High Commissioner for Operations at UNHCR.
Cross-regional strategies were encouraged to enable maximum impact and coverage of people. The challenge of sexual violence in emergency settings and gender inequalities was highlighted as a fundamental issue to be given greater focus, action and investment.
36th meeting of the PCB
Related


unaids.org
UNAIDS

Photo courtesy of UNHCR/I.Prickett
Feature Story
UNHCR: unprecedented levels of forced displacement worldwide
19 June 2015
19 June 2015 19 June 2015The number of people and families forced to flee their homes has reached an all-time high, with near...
The number of people and families forced to flee their homes has reached an all-time high, with nearly 60 million people worldwide now displaced by conflict and persecution, says a new report published by the Office of the United Nations High Commissioner for Refugees (UNHCR) for World Refugee Day on 20 June.
According to UNHCR Global trends 2014, this number is accelerating rapidly. At the end of 2014, some 59.5 million were forcibly displaced, compared to 51.2 million in 2013. Every day last year, an average of 42 500 people became refugees, asylum seekers or internally displaced. This fourfold increase in four years has largely been driven by the war in the Syrian Arab Republic, though numbers are rising across the globe as new conflicts break out or reignite.
In highlighting the unprecedented level of forced displacement and people crossing borders, UNHCR acknowledges that anxiety and intolerance towards them is also growing.
To address this, the theme of World Refugee Day 2015 is to give a human face to the crisis and show who refugees are and why they need help. By reinforcing the fact that they are ordinary people in extraordinary circumstances, UNHCR hopes to galvanize governments and the public into doing more to improve conditions, empathy and opportunities for people who are forced to move.
United Nations High Commissioner for Refugees António Guterres stressed, "With huge shortages of funding and wide gaps in the global regime for protecting victims of war, people in need of compassion, aid and refuge are being abandoned.” He added, “For an age of unprecedented mass displacement, we need an unprecedented humanitarian response and a renewed global commitment to tolerance and protection for people fleeing conflict and persecution."
A critical part of the UNHCR campaign is to tell the stories of a range of refugees and internally displaced people who are attempting to forge new lives. Several such stories revolve around people living with, or affected by HIV. People who are forcibly displaced may become more vulnerable to HIV as health services become harder to access. They might be more likely to engage in transactional sex if basic needs are not met, and rape is also often used as a weapon of war.
This was the case for Maria Kamwendo, featured by UNHCR, who was raped by rebels in the Democratic Republic of the Congo. She managed to escape and found her way to South Africa. After the shock of being diagnosed as HIV-positive, she has built a new life there and is now an HIV counsellor. “I enjoy what I do,” she says. “HIV is not a death sentence but one can be instrumental in empowering people about the disease.”
By encouraging people to get to know the stories of individual refugees, UNHCR aims to make a link between people lucky enough to have living settled lives and those who are struggling to cope with the trauma of having, through no fault of their own, to flee from their homes.
