We have bent the trajectory of the AIDS epidemic.

We have bent the trajectory of the AIDS epidemic. Now we have five years to break the epidemic or we risk the epidemic springing back even stronger. Additional resources
Financial support


28 November 2016
28 November 2016 28 November 2016Despite the progress made against HIV over the past 15 years and the availability of proven prevention and treatment methods, the annual number of new HIV infections among adults has remained static, at an estimated 1.9 million a year since 2010. Moreover, there has been resurgence of new HIV infections among key populations in some parts of the world.
Inadequate investments in prevention and unfocused investments that do not reach the most affected populations and locations are among the reasons for the prevention gap. An analysis of four countries in different regions and with different types of epidemic found that the funding of effective and focused primary HIV prevention programmes was low—6% of total HIV investments in Brazil, 4% in Cameroon, 15% in Myanmar and 10% in South Africa. Country allocations for HIV primary prevention (excluding mother-to-child transmission of HIV and voluntary HIV testing and counselling) by the United States President’s Emergency Plan for AIDS Relief and the Global Fund to Fight AIDS, Tuberculosis and Malaria have accounted for roughly 15% of total HIV expenditure.
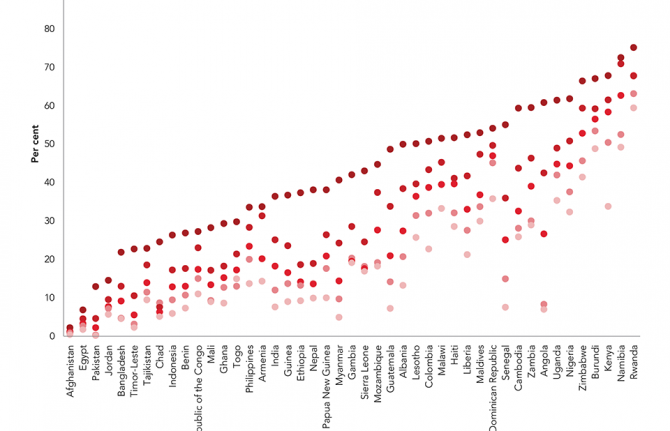
With funding for prevention falling behind funding for treatment, fewer than one in five people at higher risk of HIV infection today have access to prevention programmes. UNAIDS modelling has shown that investing around a quarter of all the resources required for the AIDS response in HIV prevention services would be sufficient to make possible a range of prevention programmes, including condom programmes, pre-exposure prophylaxis, voluntary medical male circumcision, harm reduction, programmes to empower young women and girls, and mobilizing and providing essential service packages for and with key populations.
Investing more in prevention will also support treatment programmes to achieve their targets. Prevention programmes—including providing HIV information, condom distribution and outreach to young people and key populations—are often the first entry point for individuals to HIV testing and treatment. Community peer-led prevention programmes are also critical for reducing stigma and discrimination. Meanwhile, expanded access to treatment gives people at higher risk choices and encourages them to find out their HIV status; this, in turn, provides the opportunity to retain people who test negative in ongoing prevention programmes. Reducing the number of people who acquire HIV and will need treatment makes antiretroviral therapy programmes more sustainable.
In December 2015, the UNAIDS Executive Director, Michel Sidibé, called for investing a quarter for HIV prevention. In June 2016, United Nations Member States committed in the 2016 Political Declaration on Ending AIDS to ensuring that financial resources for prevention are adequate and constitute no less than a quarter of AIDS spending globally on average.
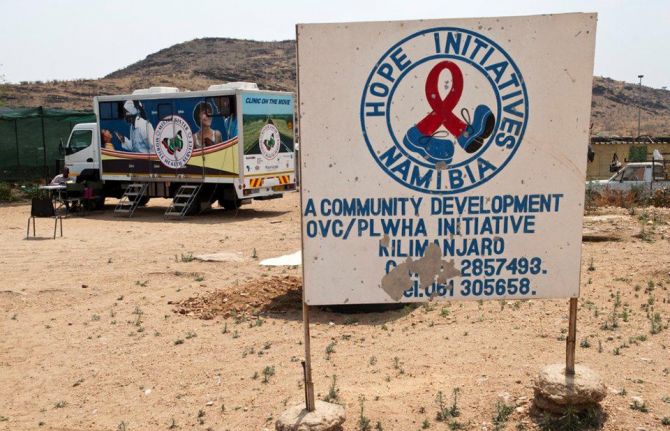
A number of countries have already taken action to increase their domestic funding for HIV prevention, including Namibia, which has committed to investing 30% of its HIV budget in preventing HIV among adults and children.
14 July 2015
We have reached a defining moment in the AIDS response. Against all odds, we have achieved the AIDS targets of Millennium Development Goal 6. AIDS changed everything. In these pages are valuable insights and ground-breaking and heart-warming experiences from the innovative and exciting work that partners, communities and countries have done and are doing in the AIDS response. There are also heart-breaking stories about the challenges that still remain. More on How AIDS changed everything
You can also view the report on Issuu Report with no annexes Annexes only

27 February 2025

18 February 2025
01 February 2025



09 June 2016
09 June 2016 09 June 2016A panel meeting at the United Nations General Assembly High-Level Meeting on Ending AIDS, being held from 8 to 10 June, warned that the global commitment to end AIDS as a public health threat by 2030 cannot be met without increased funding, more efficiency and improved programme effectiveness.
Members of the panel, which met on 8 June and was entitled “Financing the end of AIDS: the window of opportunity,” argued that greater investment in the AIDS response needs to be front-loaded in the next five years and reach the US$ 26.2 billion needed by 2020 in low- and middle-income countries. Governments and development partners must increase their investments to close the nearly US$ 7 billion gap between the resources available for HIV in 2014 and the 2020 peak. This will avoid a looming funding crisis for treatment and prevention.
According to the gathering’s political leaders, experts and representatives of international organizations and civil society, this extra funding will allow the world to meet the 2020 interim targets on the road to ending the epidemic. These targets include the 90–90–90 treatment target of 90% of people living with HIV knowing their status, 90% of people who know their HIV-positive status accessing treatment and 90% of people on treatment having a suppressed viral load, reducing new HIV infections to fewer than 500 000 and elimination of HIV-related discrimination.
It was argued that the AIDS response must spend increased funding wisely by adopting the Fast-Track approach of rapidly scaling up treatment and prevention services with more efficient and effective programmes. The panel also discussed mechanisms to facilitate development partners and low- and middle-income countries front-loading resources to reach the ultimate goal of ending the AIDS epidemic as a public health threat by 2030.
Beyond the call for more funding and better allocation of existing resources, other critical factors for the sustainability of the response were highlighted, including local production of antiretroviral medicines in Africa, improvement in the procurement of commodities through price negotiations and access and affordability of modern pharmaceuticals in all countries.
There was a strong call for the following: facilitating the transition of countries moving into higher-income brackets, including supporting community-based programmes; fully funding the needs of gay men and other men who have sex with men, people who inject drugs, sex workers, transgender people and prisoners, and particularly young people among those populations; investing in communities; and scaling up public–private partnerships.
The panel stressed forcefully that the cost of inaction for individuals, communities, countries and regions was simply too high and that the world could not afford to miss this window of opportunity to make funding sustainable and reinvigorate the HIV response over the next five years.
“Countries which can pay should do so in order for the international community to support other countries which have the will but not the financial means.”
“We need to guarantee full funding for prevention, treatment and care for people who inject drugs, gay men and other men who have sex with men, sex workers, transgender people and prisoners.” ,
“If we really want to take up the challenge of ending AIDS by 2030, we need to focus on innovative financing. Innovation financing since 2002 has yielded US$ 8 billion, including airline taxes and coupons for vaccines. It will be even more important now if we are to reach the Sustainable Development Goals.”
“The Global Fund to Fight AIDS, Tuberculosis and Malaria is everyone in this room, government, the private sector, civil society. If we all come together in the partnership that the Global Fund represents, we can absolutely end HIV, tuberculosis and malaria for good.”
“It is not just where the money comes from, it’s where the money is spent. It needs to be spent for people living with HIV, for women and for key populations. It is our lives on the line.”
“People who inject drugs have been left furthest behind in the global response to HIV. We know the HIV epidemic among people who inject drugs is driven by stigma, discrimination and violence. The lack of political willingness for harm reduction can be observed all over the world. We can virtually end AIDS among people who inject drugs by simply redirecting money from the war on drugs to harm reduction.”
“Innovation is something that we put as a top criterion for how we can deliver. We are always looking for new ideas, and I think they can come from our dedicated civil society organizations.”
“We need to see this endeavour as an investment from one generation to another. For the 2030 goals, a multisectoral approach will not allow us to reach only one objective but also to reach others. Today, crises are global and therefore require a global response.”
“For us, strengthening the health system is critical. We have a very ambitious objective to screen and treat, but with weak health systems we will be unable to achieve our goals.”
“We have a tremendously important opportunity with the replenishment of the Global Fund to Fight AIDS, Tuberculosis and Malaria. We need to look at the needs, estimate budgets based on those needs and then mobilize the resources. Everything should be driven by the analytics.”


23 October 2015
23 October 2015 23 October 2015UNAIDS has welcomed the signing of new grants between Malawi and the Global Fund to Fight AIDS, Tuberculosis and Malaria worth more than US$ 332 million. The agreement brings the total Global Fund commitment to Malawi to US$ 616 million for the period 2014-2017, the highest per capita allocation to any country globally.
The agreement will allow the further expansion of treatment and prevention programmes for all three diseases and build stronger health systems. Community based approaches to HIV prevention and programmes to diagnose new cases of tuberculosis will be scaled up. At the same time as he signed the new agreement with the Global Fund Executive Director, Mark Dybul, the President of Malawi, Peter Mutharika, committed an additional US$ 30 million from domestic resources to bolster the country’s health system.
Malawi has 1.1 million people living with HIV. It has increased the number of people accessing antiretroviral medicines from a few thousand in 2003 to more than 536 000 at the end of 2014.
The grants signed here today will strengthen the Malawi government’s efforts against AIDS, malaria and TB. These diseases are leading causes of deaths, responsible for more than two in every five deaths. The grants will be key to achieving the national strategic plans for disease control programmes such as the 90-90-90 targets set in the National Strategy for HIV and AIDS. They will also be a major contribution to achieving the Sustainable Development Goals.”
“Today is a historic moment of global solidarity and shared responsibility for Malawi. This new investment acknowledges the great work and commitment of Malawi. I have no doubt that Malawi’s strong leadership will lead to success.”
“Partnership is at the centre of what we do so it is very encouraging to see the wide array of partners that are here today working together to control the diseases in Malawi.”
14 July 2015
We have reached a defining moment in the AIDS response. Against all odds, we have achieved the AIDS targets of Millennium Development Goal 6. AIDS changed everything. In these pages are valuable insights and ground-breaking and heart-warming experiences from the innovative and exciting work that partners, communities and countries have done and are doing in the AIDS response. There are also heart-breaking stories about the challenges that still remain. More on How AIDS changed everything

27 February 2025
18 February 2025
01 February 2025
 have signed a cooperation agreement to maximize support to countries and optimize investments and impact at country level.")
09 December 2014
09 December 2014 09 December 2014UNAIDS and the Global Fund to Fight AIDS, Tuberculosis and Malaria highlighted their strong partnership to respond to infectious diseases, including HIV and tuberculosis, with a new cooperation agreement to help countries achieve the Fast-Track Targets to end the AIDS epidemic as a global health threat by 2030.
At the core of the agreement is an improved way of collaborating that strengthens coordination mechanisms, information-sharing at all levels and mutual accountability.
The UNAIDS Fast-Track approach emphasizes the need to focus on the counties, cities and communities most affected by HIV and recommends that resources be concentrated on the areas with the greatest impact. The new agreement will focus on maximizing support to countries and optimizing investments and impact at the country level.
Cooperation areas include strengthening strategic investments, jointly leveraging political commitment and supporting meaningful country dialogues with all stakeholders—including civil society and communities—to ensure that no one is left behind.
The new agreement will leverage the strengths of both organizations in providing technical support to countries and coordination throughout the grant cycle. Special emphasis will be placed on data collection, analysis and identification of gaps in the epidemic and the response, including on countries’ enabling environments, equity in access to services, human rights, gender and key populations at higher risk.
The new cooperation agreement replaces a memorandum of understanding signed in 2008. The agreement will be revisited at the end of 2016.
“This agreement with the Global Fund reinforces our strong relationship and will advance our joint efforts to end the AIDS epidemic by 2030. UNAIDS is fully mobilized to support the Global Fund’s New Funding Model, which will empower countries to be even more effective, inclusive, grounded in human rights and sustainable in their AIDS responses.”
“Working together, we can achieve even more for people affected by HIV. This agreement captures the spirit of collaboration, which we already do, and will help take us to an even greater level.”
We have bent the trajectory of the AIDS epidemic. Now we have five years to break the epidemic or we risk the epidemic springing back even stronger. Additional resources

18 August 2014
18 August 2014 18 August 2014Now a 19-year-old university student in South Africa, Noxolo Myeketsi started receiving a social welfare grant in 2005. Part of a state-run programme to assist poor households, the cash transfers allowed her to stay in school and her grandmother to buy food and pay their bills.
The grant changed Noxolo’s life for the better. Other girls turned to having sex, often with older men, in exchange for basic needs, and potentially exposed themselves to sexually transmitted infections and HIV.
“I believe that without the grant assistance, I would not have been able to make healthy decisions in my life. Maybe I would have ended up being a sugar daddy’s girl, like others from my area, or ended up contracting HIV,” Noxolo said.
Social protection schemes, including financial incentives, can make a difference in a number of ways. The World Bank reports that, globally, there is strong evidence that cash transfers improve the education, health and lifelong income of beneficiaries.
“Cash transfer programmes work for HIV prevention and a host of other human development outcomes as well, and they are scalable,” said David Wilson, Director of the World Bank’s Global HIV/AIDS Program.
Studies conducted in South Africa show that small cash grants provided to poor households allow teenage girls to make safer sexual choices and can significantly reduce the number of new HIV infections. When psychosocial care and support are added to the cash, the results for girls are even better.
At the UNAIDS Programme Coordinating Board (PCB) meeting held in Geneva in July a thematic session was organized on addressing the social economic drivers of HIV through social protection, at which Noxolo spoke about the positive impact grants can have.
Following up on the PCB meeting, UNAIDS and the World Bank pledged to assist governments in the process of scaling up social protection programmes, including cash transfers, for HIV prevention in eastern and southern Africa, covering Botswana, Kenya, Lesotho, Malawi, South Africa, Swaziland, United Republic of Tanzania and Zambia.
“It is befitting that South Africa is the centre of the initiative because the country accounts for 23% of sub-Saharan Africa’s new HIV infections, 18% of the global HIV burden and has one of the world largest social protection programmes,” said Benjamin Ali, UNAIDS Country Director for South Africa.
Countries and partners will be urged to collaborate in a comprehensive review of social protection systems. Proposals to make such systems HIV sensitive include modifying age bands and other inclusion criteria to ensure that the groups most affected and at risk of HIV infection are covered, providing some cash directly to girls and young women and linking cash incentives to their adherence to HIV prevention and treatment programmes.

25 February 2025