Community mobilization


Feature Story
Changing the landscape of community engagement in the HIV response in Indonesia
22 July 2021
22 July 2021 22 July 2021“Communities must be allowed to sit in the driver’s seat and take control of their lives. They are not passengers that sit idle, but leaders capable of making changes,” said Aditya Wardhana, the Executive Director of the Indonesian AIDS Coalition (IAC). This is the motto that he lives by, a motto that drives the work of IAC and how communities and civil society are meaningfully engaged in the HIV response in Indonesia.
IAC is a community-led organization based in Jakarta and was recently appointed the second community Principal Recipient to implement the Global Fund to Fight AIDS, Tuberculosis and Malaria’s (Global Fund) grant for HIV in Indonesia for 2022–2023—a feat, since only a handful of community-based organizations nationally or regionally hold Global Fund Principal Recipient status.
“Often, communities are seen as beneficiaries of programmes or as patients, not as decision makers. The IAC has always strived to shake up this dynamic. We believe that being a Principal Recipient will give us greater control over the issues that impact our communities and will set the direction of the national HIV response that puts communities at the centre of it,” explained Mr Wardhana.
In Indonesia, there are still significant gaps in the HIV response. Treatment coverage is low, with only 26% of people living with HIV on treatment, prevention is still lagging and stigma and discrimination remains high. IAC has identified three priorities to improve the HIV response in Indonesia, which include recognizing community health workers as health workers, creating more sustainable financing to reduce reliance on external donors and reforming laws and policies that discriminate and lack redress mechanism for victims of discrimination.
Networks of people living with HIV deliver life-changing services to those most affected and provide support for adherence to treatment, prevention and other essential health services. The involvement of civil society has been crucial in successfully advocating for sustainable financial resources, improving HIV programming and advancing human rights.
Over the next couple of years, IAC will work on these priority issues with the support of civil society organizations, United Nations partners and other stakeholders. IAC will continue to manage the human rights and community system strengthening programme, supported by the Global Fund and the Ministry of Health. Community system strengthening and community-led monitoring are integral parts of the HIV response. The programme ensures that community-based organizations play an active role in monitoring access to services, community programme quality assurance and human rights violations.
Since the organization’s foundation, the UNAIDS Country Office for Indonesia has been an ally and key partner, supporting IAC throughout the Principal Recipient selection process. “We know how important the role of communities is at all levels of the HIV response. We will continue to support IAC by providing technical assistance and capacity-building, working in collaboration to promote the meaningful engagement of communities and civil society in the HIV response,” said Krittayawan Boonto, the UNAIDS Country Director for Indonesia.
IAC, with support from the United Nations Population Fund in Indonesia, will soon establish a peer-led HIV prevention programme for female sex workers, offering differentiated service delivery to increase the uptake of HIV prevention services. Through the programme, they will also empower communities through capacity-building initiatives to drive the greater involvement of civil society in decision-making, especially in forming policies that directly impact the health and well-being of communities and vulnerable populations. Moreover, IAC plans to integrate gender-based violence screening into its outreach programmes. A human rights-based approach is essential to ending AIDS as a public health threat. This approach will create an enabling environment for successful HIV responses and affirms the dignity of people living with or vulnerable to HIV.
IAC will be responsible for managing US$ 17 million to implement the above programmes, with eight organizations across Indonesia as subrecipients.
“We will dive deep into these challenges and hopefully change the landscape of the HIV response. We believe that a more participatory approach will re-energize communities and remind them why HIV is still important and how programmes designed by communities for communities can save lives. This is what we will work towards; this is how we will end AIDS by 2030,” said Mr Wardhana.
Our work
Region/country
Related



Feature Story
Putting people and communities at the centre of the HIV response
10 June 2021
10 June 2021 10 June 2021Communities living with and affected by HIV, including communities of key populations, are the backbone of the HIV response. They have campaigned for their rights, expanded the evidence base for effective action against HIV, supported the design and implementation of programmes and enhanced the reach and quality of health services. They ensured that the greater involvement of people living with HIV principle became an organizing norm for HIV programmes and that rights-based approaches were widely adopted.
A panel, Putting People and Communities at the Centre of the Response to AIDS, held on the sidelines of the United Nations High-Level Meeting on AIDS on 9 June, saw a high-level discussion on the opportunities and challenges for moving towards the global AIDS targets and realizing the political commitments and policy adaptations needed to support community-led responses as the world moves towards ending AIDS by 2030, and does so in the context of COVID-19.
The panel discussed supporting key population-led, women-led and other community-led responses, new priorities emerging from the community-led response to COVID-19 and fair payment for the community workforce, in particular for women living with HIV and women from key and vulnerable populations.
The panellists heard that more than three decades of experience has clearly shown that communities are at the centre of efforts to end AIDS as a public health threat, but their significant contribution is too often set aside or made more difficult by politicians or public health officials who have little or no knowledge of the lives and experiences of the people they are charged to serve.
They also heard that the response to the COVID-19 pandemic has further underscored the importance of communities in navigating difficult and rapidly changing environments and in reaching affected communities with essential services, such as COVID-19 testing and vaccination and HIV prevention, testing and treatment and other health and social services.
During their discussions, all panellists stressed that communities can deliver when there is an enabling legal environment, operating space for civil society organizations and funding and capacity-building.
Quotes
“The government needs to implement the policies and remove the legal barriers that can enable implementation of the required initiatives. There need to be financing mechanisms and technical support for community-led services, as this is crucial to ensure the quality and sustainability of services, and trusting multisectoral partnerships among stakeholders need to be forged so that there is a united front towards achieving the same goal by putting people at the centre of implementation.”
“Whilst communities are best placed to reach their members, governments have the capacity and resources to support and accelerate progress by ensuring a safe space for civil society through law and policy reform to decriminalize key populations, reduce discrimination and prevent hate crimes, to enable everyone to live peacefully and to enjoy their human rights.”
“Lessons learned from community-led and centred service delivery have strongly shown us that communities have the experience, ability and knowledge on how to best serve their own communities. Communities have a lot to teach us.”
“We cannot end AIDS without investing in harm reduction, community-led responses and the rights of people who use drugs.”
Our work
Related


Feature Story
UNAIDS is deeply saddened by the death of Manuel da Quinta, a great professional and activist in the response to HIV and the promotion of human rights and equality
14 June 2021
14 June 2021 14 June 2021The UNAIDS family is deeply saddened by the death from COVID-19 of our dear colleague and friend, Manuel de Quinta. We offer our deepest condolences to his husband Ricardo and to his family and friends in general.
Since 2017, Manuel worked as a UNAIDS Community Support and Human Rights Adviser for the multicountry UNAIDS Office for Argentina, Chile, Paraguay and Uruguay. But many of us knew him in the many roles he held and the tremendous work he did around the world as part of the UNAIDS family for more than 24 years advocating for the rights and leadership of people living with HIV and the populations most vulnerable to HIV, including the lesbian, gay, bisexual, transgender and intersex community, migrants and refugees, sex workers, indigenous peoples and young people.
Manuel represented the essence of UNAIDS’ mission and vision and the reason why all of us get up every day to fulfil our duties and purpose. As a strong advocate for human rights and social equality, he always stood up against all forms of injustice, including internally at UNAIDS, where for many years he was the Chair of the UNAIDS Staff Association.
Manuel was an HIV activist since 1990 and accumulated a vast experience of community work with organizations working on behalf of people living with HIV in several countries in Africa, Asia and Latin America.
He joined UNAIDS in 1997, starting in the Communications Department, managing multimedia projects on HIV. Later, in 2005, he co-founded UN Plus, an initiative that brings together United Nations system staff living with HIV. Since then, he has worked in UNAIDS teams in Geneva, Bangkok, Dakar and Buenos Aires.
Manuel was a person with great positive energy, an enormous willingness to make even the impossible possible, bringing a deep passion to everything he undertook. He was also a loyal friend to many of us.
Manuel left us at the early age of 59 years and will be deeply missed.
We wish to express our deep sorrow at his passing and to reiterate our solidarity and warmth to the great community that has worked with Manuel in the HIV response over so many years, and to all those who have known him around the world and who mourn his departure.


Feature Story
What responses to HIV and COVID-19 in Asia and the Pacific led by civil society can teach us
11 June 2021
11 June 2021 11 June 2021COVID-19 continues to threaten the gains made in the HIV response and has brought inequalities to the forefront, but civil society and community-based organizations in Asia and the Pacific have been quick to respond to the pandemic. From the start, networks of people living with HIV and key populations responded to the global health crisis by coming up with innovative courses of action.
A side event organized on the margins of the United Nations High-Level Meeting on AIDS showcased best practices of community-led responses to COVID-19 and HIV prevention in Asia and the Pacific.
It was noted that, since the onset of the COVID-19 pandemic, key population networks have rapidly mobilized volunteers and partners to assist people affected by COVID-19, ensured the continuity of HIV services and found new ways to adapt to the new normal with online-based interventions.
For example, the Asia Pacific Network of Sex Workers responded to the pandemic by modifying its existing programmes to meet the urgent needs of the sex worker community, such as by reallocating funds to subsidize transport costs for sex workers living with HIV to ensure their access to HIV treatment services.
Other regional networks, such as the Asia Pacific Transgender Network, the Asia Pacific Network of People Living with HIV and Youth LEAD, established emergency relief funds to provide emergency food supplies, housing and rent, transport, protective gear, including personal protective equipment, masks, sanitizer and sanitary products for the most affected communities.
In several countries, community-led organizations of people who use drugs delivered door-to-door provisions of antiretroviral therapy and harm reduction services, including opioid substitution therapy and sterile needles and syringes. These experiences have been compiled by the Asia Pacific Network of People who Use Drugs in a best practice report to advocate for the full and equal participation of people who use drugs within the HIV response.
The panellists also heard about the Australian Federation of AIDS Organisations, which in its national and community-led responses has been supporting community-based HIV testing, working directly with clinics run by the community for the community. Also, APCOM, a regional network for gay men and other men who have sex with men based in Bangkok, Thailand, implemented a condom promotion campaign during the COVID-19 pandemic, known as #PartyPacks, where key populations can order online (for free) packages containing condoms, lubricant and information on harm reduction.
The speakers agreed that service delivery needs to be modernized, domestic investment should be increased and services led by key populations should be integrated into national health systems.
The panellists highlighted that dealing with the colliding pandemics of HIV and COVID-19 requires working in unison and solidarity.
Quotes
“While the journey has not been smooth, one of Australia’s key learnings is that the voices of the community are essential. Communities of people living with HIV and those populations at high risks and young people—communities who, if we are to really make a difference, must have a central role in sharing the view of those most affected by HIV with national governments.”
“Thailand’s effort on HIV/AIDS is one area where civil society plays a particularly vibrant role in our country. We recognized that the collaboration of different sectors, especially civil society and the network of people living with HIV, is one of the most important factors in Thailand’s success in controlling the spread of HIV and AIDS.”
“The valuable experiences of communities reflect their long-standing active participation in the response to the HIV epidemic. This is exhibited in the way they continue to innovate at the forefront of the response to HIV and, most recently, address the intersectionality that emerged out of having to respond to the impact of COVID-19 as well.”
“Key populations are widely recognized as the pioneers and leaders of the HIV response. Since the emergence of HIV, key populations have led the way in pioneering effective prevention responses, sharing their knowledge and skills with the community as well as providing essential care and support.”
“Community-led organizations are the most effective way to reach sex workers during emergencies as they are capable of providing therapy assessment, identifying priority areas and allocating the resources for various types of relief for sex workers. This is facilitated by an established peer-to-peer model that is led by the trust and knowledge of peer outreach programmes, which is also able to deliver emergency aid to the most in need.”
Our work
Region/country
Related



Press Release
New global pledge to end all inequalities faced by communities and people affected by HIV towards ending AIDS
08 June 2021 08 June 2021World leaders agree to reduce the annual number of new HIV infections to under 370 000 and AIDS-related deaths to 250 000, eliminate new HIV infections among children, end paediatric AIDS and eliminate all forms of HIV-related discrimination by 2025. They also committed to providing life-saving HIV treatment to 34 million people by 2025.
NEW YORK, 8 June 2021—United Nations Member States adopted a set of new and ambitious targets in a political declaration at the United Nations General Assembly High-Level Meeting on AIDS, taking place in New York, United States of America. If the international community reaches the targets, 3.6 million new HIV-infections and 1.7 million AIDS-related deaths will be prevented by 2030.
The political declaration calls on countries to provide 95% of all people at risk of acquiring HIV within all epidemiologically relevant groups, age groups and geographic settings with access to people-centred and effective HIV combination prevention options. It also calls on countries to ensure that 95% of people living with HIV know their HIV status, 95% of people who know their status to be on HIV treatment and 95% of people on HIV treatment to be virally suppressed.
“In this Decade of Action, if we are to deliver the 2030 Agenda for Sustainable Development all Member States must recommit to ending the AIDS epidemic by 2030,” said Volkan Bozkir, the President of the United Nations General Assembly.
“To end AIDS, we need to end the intersecting injustices that drive new HIV infections and prevent people from accessing services,” said Amina J. Mohammed, Deputy Secretary-General of the United Nations.
The political declaration notes with concern that key populations—gay men and other men who have sex with men, sex workers, people who inject drugs, transgender people and people in prisons and closed settings—are more likely to be exposed to HIV and face violence, stigma, discrimination and laws that restrict their movement or access to services. Member States agreed to a target of ensuring that less than 10% of countries have restrictive legal and policy frameworks that lead to the denial or limitation of access to services by 2025. They also committed to ensure that less than 10% of people living with, at risk of or affected by HIV face stigma and discrimination by 2025, including by leveraging the concept of undetectable = untransmittable (people living with HIV who have achieved viral suppression do not transmit HIV).
“I would like to thank Member States. They have adopted an ambitious political declaration to get the world back on track to ending the AIDS pandemic that has ravaged communities for 40 years,” said Winnie Byanyima, the UNAIDS Executive Director.
Expressing concern at the number of new HIV infections among adolescents, especially in sub-Saharan Africa, a commitment was made to reduce the number of new HIV infections among adolescent girls and young women to below 50 000 by 2025. Member States committed to eliminate all forms of sexual and gender-based violence, including intimate partner violence, by adopting and enforcing laws that address the multiple and intersecting forms of discrimination and violence faced by women living with, at risk of and affected by HIV. They pledged to reduce to no more than 10% the number of women, girls and people affected by HIV who experience gender-based inequalities and sexual and gender-based violence by 2025. In addition, commitments were made to ensure that all women can exercise their right to sexuality, including their sexual and reproductive health, free of coercion, discrimination and violence.
Countries were also urged to use national epidemiological data to identify other priority populations who are at higher risk of exposure to HIV, which may include people with disabilities, ethnic and racial minorities, indigenous peoples, local communities, people living in poverty, migrants, refugees, internally displaced people, men and women in uniform and people in humanitarian emergencies and in conflict and post-conflict situations. Countries also committed to ensure that 95% of people living with, at risk of and affected by HIV are protected against pandemics, including COVID-19.
“The stark inequalities exposed by the colliding pandemics of HIV and COVID-19 are a wake-up call for the world to prioritize and invest fully in realizing the human right to health for all without discrimination,” said Ms Byanyima.
Member States also committed to increase and fully fund the AIDS response. They agreed to invest US$ 29 billion annually by 2025 in low- and middle-income countries. This includes investing at least US$ 3.1 billion towards societal enablers, including the protection of human rights, reduction of stigma and discrimination and law reform. They also committed to include peer-led HIV service delivery, including through social contracting and other public funding mechanisms.
Calling for expanding access to the latest technologies for tuberculosis (TB) prevention, screening, diagnosis, treatment and vaccination, Member States agreed to ensure that 90% of people living with HIV receive preventive treatment for TB and reduce AIDS-related TB deaths by 80% by 2025. Countries also committed to ensure the global accessibility, availability and affordability of safe, effective and quality-assured medicines, including generics, vaccines, diagnostics and other health technologies to prevent, diagnose and treat HIV infection, its coinfections and other comorbidities through the use of existing flexibilities under the Agreement on Trade-Related Aspects of Intellectual Property Rights (TRIPS) and ensure that intellectual property rights provisions in trade agreements do not undermine the existing flexibilities as outlined in the Doha Declaration on the TRIPS Agreement and Public Health.
“The AIDS response is still leaving millions behind—LGBTI people, sex workers, people who use drugs, migrants and prisoners, teenagers, young people, women and children—who also deserve an ordinary life, with the same rights and dignity enjoyed by most people in this room,” said Yana Panfilova, a woman living with HIV and member of the Global Network of People Living with HIV.
The high-level meeting is being attended in-person and virtually by heads of state and government, ministers and delegates in New York, people living with HIV, civil society organizations, key populations and communities affected by HIV, international organizations, scientists and researchers and the private sector. UNAIDS supported regional consultations and the participation of civil society in the high-level meeting. Civil society organizations called on Member States to adopt a stronger resolution.
“While we have made some significant progress as a global community, we are still missing the mark and people are paying the price with their lives. There’s one single reason we are missing our goal: it’s inequality,” said Charlize Theron, Founder of the Charlize Theron Africa Outreach Project and a United Nations Messenger of Peace.
Member States also committed to support and leverage the 25 years of experience and expertise of the Joint United Nations Programme on HIV/AIDS (UNAIDS) and committed to fully fund the programme so that it can continue to lead global efforts against AIDS and support efforts for pandemic preparedness and global health.
In accordance with the Global AIDS Strategy 2021–2026: End Inequalities, End AIDS, adopted by consensus on 25 March 2021 by the UNAIDS Programme Coordinating Board, as well as the report of the United Nations Secretary-General, Addressing Inequalities and Getting Back on Track to End AIDS by 2030, issued on 31 March 2021, UNAIDS would have welcomed even stronger commitments on comprehensive sexuality education, sexual and reproductive health and rights, and sexual orientation and gender identity, unqualified acceptance of evidence-based HIV prevention options, such as harm reduction, a call for the decriminalization of the transmission of HIV, sex work, drug use and laws that criminalize same-sex sexual relationships and further flexibilization of intellectual property rules for access to life-saving medicines, vaccines and technologies.
In 2020, 27.4 million of the 37.6 million people living with HIV were on treatment, up from just 7.8 million in 2010. The roll-out of affordable, quality treatment is estimated to have averted 16.2 million deaths since 2001. AIDS-related deaths have fallen by 43% since 2010, to 690 000 in 2020. Progress in reducing new HIV infections has also been made, but has been markedly slower—a 30% reduction since 2010, with 1.5 million people newly infected with the virus in 2020, compared to 2.1 million in 2010.
UNAIDS
The Joint United Nations Programme on HIV/AIDS (UNAIDS) leads and inspires the world to achieve its shared vision of zero new HIV infections, zero discrimination and zero AIDS-related deaths. UNAIDS unites the efforts of 11 UN organizations—UNHCR, UNICEF, WFP, UNDP, UNFPA, UNODC, UN Women, ILO, UNESCO, WHO and the World Bank—and works closely with global and national partners towards ending the AIDS epidemic by 2030 as part of the Sustainable Development Goals. Learn more at unaids.org and connect with us on Facebook, Twitter, Instagram and YouTube.
Contact
UNAIDS GenevaSophie Barton-Knott
tel. +41 79 514 68 96
bartonknotts@unaids.org
UNAIDS Media
tel. +41 22 791 4237
communications@unaids.org
Watch Winnie Byanyima's full speech
 and moderated by the Caribbean Community (CARICOM) Assistant Secretary-General, Douglas Slater")
, Diana Weekes noted that key structural barriers continue to block access to HIV prevention, treatment and care services.")



Feature Story
Caribbean stakeholders call for focus on key populations and community-led approaches to HIV and COVID-19
08 June 2021
08 June 2021 08 June 2021Caribbean partners from governments, civil society and the development community met on 7 June to discuss regional priorities for the 2021 United Nations High-Level Meeting on AIDS and its resulting political declaration. The virtual Caribbean Caucus was hosted by the Pan Caribbean Partnership against HIV/AIDS (PANCAP) and moderated by the Caribbean Community (CARICOM) Assistant Secretary-General, Douglas Slater.
The PANCAP Director, Rosmond Adams, noted that the Caribbean has made significant progress in key aspects of the HIV response. Eight countries and territories have been validated by the World Health Organization for eliminating vertical HIV and syphilis transmission. And between 2010 and 2020, AIDS-related deaths in the region fell by half (51%).
But to get on track to end AIDS by 2030, he said Caribbean countries must step up the pace around prevention, testing, treatment, care and ending stigma and discrimination. By 2020, 82% of people living with HIV in the region were diagnosed. Two thirds (67%) of all people living with HIV were on treatment and 59% were virally suppressed.
While new HIV infections have fallen by 28% since 2010, the rate of decline is too slow. Overall, members of key population communities and their partners accounted for 60% of new HIV infections in 2020. Around one third of new HIV infections were among young people aged 15–24 years.
Speaking on behalf of the Caribbean Regional Network of People Living with HIV (CRN+), Diana Weekes noted that key structural barriers continue to block access to HIV prevention, treatment and care services. These include “stigma and discrimination … lack of privacy, breach of confidentiality and limited redress” when people’s rights have been violated. She noted that no country in the region has adopted the CARICOM model antidiscrimination legislation, which was developed almost a decade ago. CRN+ called for greater emphasis on policy and legislative changes as well as community-led responses to address these structural barriers.
Ivan Cruickshank, the Executive Director of the Caribbean Vulnerable Communities Coalition, pointed to regional data that show that HIV disproportionately affects key populations, including gay men and other men who have sex with men, transgender people, sex workers and people who use drugs.
“According to the latest UNAIDS report, nations with progressive laws and policies, as well as robust and inclusive health systems, have had the best HIV outcomes. We must therefore create inclusive societies in which people are confident in their ability to seek medical treatment and exercise their social and economic rights. We must go beyond declarations, to remove laws that continue to criminalize communities and limit young people’s access to sexual and reproductive health and rights,” Mr Cruickshank said.
The Guyana Health Minister and Caribbean representative on the UNAIDS Programme Coordinating Board, Frank Anthony, reaffirmed the region’s commitment to the HIV response, saying that “governments in the region stand ready to do their part in ending AIDS by 2030.”
He pointed to longstanding challenges in the region, such as “removing the legal obstacles that foster discriminatory practices” and “prevention sustainability.” But he also emphasized the new threat posed by COVID-19, noting that “finite financial resources had to be reprogrammed to meet these urgent demands.” He called for increased vaccine equity and a review of plans to transition countries in the region away from international HIV funding.
“We must use the platform available to us at this United Nations high-level meeting to ensure that we highlight our vulnerabilities to the HIV epidemic and the COVID-19 pandemic,” he said.
During discussions, civil society participants also emphasized the profound negative impact of COVID-19 containment measures on lives and livelihoods. They said there was an additional need for solutions to provide nutrition, mental health and financial support to people living with HIV and members of key population communities.
The Director of the UNAIDS New York Liaison Office, César Núñez, noted that in the response to both HIV and COVID-19, the role of communities is clear.
“The response must include a key role for civil society at the table when frameworks are being put together and implemented,” he said.
Mr Núñez ended by calling for CARICOM’s support in securing an ambitious, action-oriented and laser-focused political declaration.
Region/country
Related

Feature Story
Hearing civil society’s voice on the High-Level Meeting on AIDS
04 June 2021
04 June 2021 04 June 2021At the United Nations High-Level Meeting on AIDS, which will take place from 8 to 10 June, Member States will adopt a new political declaration to bring the HIV response back on track. After the uneven progress made in the HIV response since the 2016 United Nations High-Level Meeting on Ending AIDS, this year’s high-level meeting will be the springboard for a decade of action to reduce inequalities and root out the social determinants that fuel the HIV epidemic.
In order to find out more about civil society’s aspirations and hopes for the high-level meeting and political declaration, UNAIDS talked to two civil society representatives, both of whom are living with HIV. Jacqueline Rocha Côrtes (JRC) is from the National Movement of Women Living with HIV/AIDS (MNCP/Brazil), the Latin American and the Caribbean Movement of Positive Women (MLCM+) and the National Institute of Reassigned Women (INAMUR/Brazil). Andrew Spieldenner (AS) is the Executive Director of Mpact. Both are members of the Multistakeholder Task Force to the HLM and were involved in drafting the 2021 high-level meeting civil society declaration, in which civil society organizations urge Member States to focus efforts and resources where they are most needed and to adopt a political declaration that explicitly recognizes who is most at risk of HIV and acknowledges why this is so, to commit to fully fund and support effective HIV responses and to hold Member States accountable for their actions.
What is the purpose of the civil society declaration you released ahead of the high-level meeting?
JRC: The civil society declaration has several purposes. First of all, to bring together the main inputs given by civil society globally on the desired content of the 2021 political declaration on AIDS. Secondly, the civil society declaration serves as a tool to mobilize community efforts locally and regionally and to harmonize and sharpen our positions in order to build a stronger community position on our demands worldwide.
AS: The civil society declaration released ahead of the high-level meeting is a clear statement of the values, concerns and needs of our communities. Where Member States might be more concerned with politics, civil society continues to elevate and centre those most impacted by HIV—the same populations most often marginalized by governments through punitive laws and policies. As civil society, we want to ensure that Member States understand where we stand, in the hope that they support our work and communities in the development of the political declaration.
What are the major asks from civil society to Member States?
JRC: The major asks from the civil society declaration, from my personal perspective, are to show and remind Member States how strong we are and of our ability to mobilize and guide what is needed to end AIDS. It is an opportunity to show that we, the communities, are alive and attentive, even more so during times like this, where the COVID-19 pandemic has had such a negative impact on the response to AIDS. It is also a call to international and multilateral organizations.
AS: We want Member States to recognize the disproportionate impact of HIV on sex workers, people who use drugs, transgender people and gay and bisexual men and to centre the needs of key populations in the HIV response. We want Member States to support the delivery of necessary HIV interventions, such as comprehensive sexuality education, harm reduction in all its forms and HIV prevention and treatment. We want Member States to protect sexual and reproductive health and rights. We want Member States to be flexible with the Trade-Related Aspects of Intellectual Property Rights (TRIPS) with HIV technologies and to fully fund the HIV response.
What are the expectations of communities and civil society organizations for the upcoming high-level meeting and new political declaration?
JRC: In the political declaration, we expect to see a minimum standard of progressive broad language that includes everyone in order to make it clear that, when we refer to the response to AIDS, we are referring to human rights, the flexibility of trade agreements, the financing of the AIDS response, the community-led responses, the reduction and elimination of gender-based violence. We expect the political declaration to include firm commitments to fulfil the many goals established in the 2016 political declaration and in other political declaration that have not yet been met, as well as the most recent priorities established by the UNAIDS Global AIDS Strategy 2021–2026, agreed by many countries, which calls for the elimination of inequalities to end AIDS by 2030.
We also hope that conveniently politically correct technical language won’t serve as a veil to cover particular interests, leaving aside issues such as sexual and human diversity, sexual health and reproductive rights and the reduction and gradual elimination of punitive laws that further stigmatize people and punish citizens, who are often imprisoned or killed simply because they exist as they are.
AS: As civil society and communities, we expect Member States to support the Global AIDS Strategy 2021–2026. We understand that some Member States will be against the language describing key populations, as well as against key HIV interventions, including harm reduction, comprehensive sexuality education and TRIPS flexibilities. We hope that Member States can seek compromise to embrace and support what’s necessary to move forward in the HIV response.
Some Member States are still reticent to advance the agenda when it comes to key populations, drug use and the criminalization of sex work. What would be your message to them?
JRC: My message to them is that whether they accept it or not, humanity will not be linear like some of their political and economic projects and even social projects that try to dictate the course of human lives, over which the authorities have no governability or rights. In the same way that United Nations Member States refer to national sovereignty on whether to adopt or not certain measures, people have an inalienable autonomy to decide what is best for their lives and how they want to live.
It is imperative that Member States recognize the existence and rights of key populations.
As a reassigned transsexual woman living with HIV for 27 years, I cannot help but state that if we want to end inequalities we will necessarily have to approach and embrace human diversity.
AS: After 40 years of HIV, the disproportionate burden of HIV remains on key populations, including people who use drugs, sex workers, gay and bisexual men and transgender people. We cannot end the HIV epidemic if we do not centre the needs of key populations, including the greater involvement of people living with HIV. If Member States continue to ignore our needs, marginalize our communities and legislate against us, then the HIV epidemic will continue unabated, no matter the advances in HIV technologies.
Once the political declaration has been adopted, what will be the role of civil society in making it a reality on the ground?
JRC: We will do what we have always done—we will advocate and influence politics. We will monitor and mobilize, fight, carry out community-led work and provide community responses, build and act with solidarity, respect the internal dynamics of the various sectors, including the governments, but act on our rights and demand that our governmental authorities to do their work and comply with their commitments and duties.
And we count on UNAIDS, one of our most valuable partners, and on other United Nations agencies.
AS: The global key population networks have been advocates for community-led responses and accountability mechanisms. With the support of multilateral and philanthropic funding, we will continue to support grass-roots local and regional efforts. Unfortunately, with shrinking civil society space and funding, this will be a challenge. We need multilateral and philanthropic support in order to continue this role.
Our work
Related
Feature Story
Republic of Moldova is pioneering high-tech community-led monitoring
31 May 2021
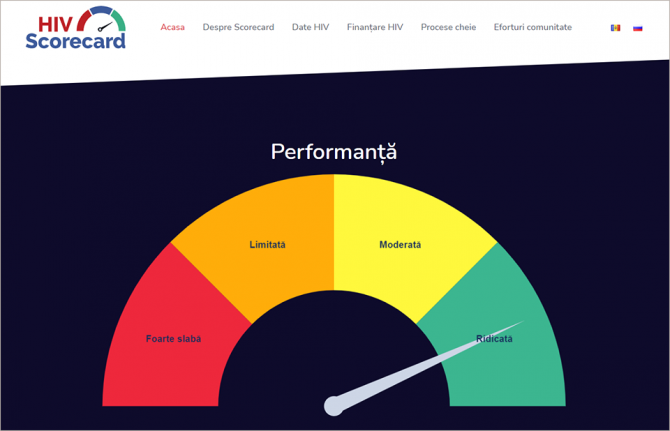
31 May 2021 31 May 2021The Republic of Moldova has launched an online platform, ScorecardHIV, to measure progress in the country's HIV response.
The new tool includes indicators and data on epidemiology, funding and procurement, programmes, human rights and community-led services. It will allow governmental institutions, health programme managers, HIV service organizations, communities and other stakeholders to track the progress and assess the effectiveness of HIV programmes in the country. A data filtering system allows the customization of indicators in accordance with the user’s interests and needs.
“The ministry will take the lead and provide political support to make sure further implementation of the tool is as effective, systematic and sustainable as possible,” said Denis Chernelya, the Secretary of State at the Ministry of Health, Labour and Social Protection. “It will be an extremely useful tool for internal monitoring as well as for understanding the main factors that contribute or impede the achievement of the set targets.”
The scorecard aims to ensure open, transparent and collective state and community-led monitoring of the HIV response. It will contribute to real-time data analysis and a rapid evidence-informed HIV response. The platform was developed by the UNAIDS Country Office for the Republic of Moldova together with the Positive Initiative nongovernmental organization and other local civil society organizations under the auspices of the Ministry of Health, Labour and Social Protection and the National Programme for the Prevention and Control of HIV/AIDS and Sexually Transmitted Infections.
The indicator map of the scorecard, which was discussed and agreed upon by all stakeholders, is sourced from the national HIV programme, ministries and government agencies and civil society organizations and is updated regularly, depending on the selected indicator—once a month, quarterly or half yearly. The platform allows data to be aggregated from different applications and sources and visualizes progress and failures in HIV programme implementation almost in real time. A task force consisting of several community organizations will update the scorecard and periodically review it.
The scorecard demonstrates how real-time data, technology and innovation can be of service for evidence-informed decisions and can strengthen cooperation between the government and communities.
“If we need to make decisions today, then we need the most recent data today. All our efforts were aimed at digitizing all possible processes, creating an infrastructure and finding IT solutions where everything can be accumulated, and then creating an analytics tool that will show us the main indicators,” said Ruslan Poverga, the Director of the Positive Initiative.
“We welcome such an important development in the Republic of Moldova,” said Alexander Goliusov, Director, a.i., of the UNAIDS Regional Support Team for Eastern Europe and Central Asia. “The scorecard was developed in line with the core principles of the new global AIDS strategy, including significant and measurable participation of civil society, a national response based on the available scientific evidence and technical knowledge, and respect for human rights and gender equality. I believe that the ability to track progress in real time, identify priority areas for rapid measures and political will and buy-in by the county’s national authorities will enable the Republic of Moldova to significantly accelerate progress towards the goal of ending AIDS by 2030.”
Learn more
Region/country
Related


 association holds up a message on a placard at the GALZ drop-in centre in Mutare, Zimbabwe.")
 association at the GALZ drop-in centre in Mutare, Zimbabwe.")
Feature Story
#NotYetUhuru: 60-year-old Patson Manyati reflects on being gay in Zimbabwe*
17 May 2021
17 May 2021 17 May 2021Patson Manyati cuts an awkward and lonely figure in a room bustling with young people in their twenties. His elegant poise, greying beard and baby blue shirt place him at least 40 years too old for this scene.
Mr Manyati is on one of his first visits to the drop-in centre of Gays and Lesbians of Zimbabwe (GALZ) in Mutare, in eastern Zimbabwe. GALZ is a membership-based association that promotes, represents and protects the rights of lesbian, gay, bisexual, transgender and intersex (LGBTI) people in Zimbabwe.
While Mr Manyati may look out of place, being at GALZ is the most “comfortable” he has ever felt as a gay man living in Zimbabwe in his 60 years.
“When I see people like me, I feel very happy,” says Mr Manyati in his musical, soft-spoken voice. His eyes don’t stop shimmering while he talks. Remarkable for someone who has grown up around pervasive homophobia. The kind of homophobia that, as recently as 2017, saw the former president describe gay people as, “worse than dogs and pigs.”
GALZ maintains that the hatred and fear caused by the late president’s particular brand of homophobia, “is still being felt in Zimbabwe today.”
While being at GALZ makes him happy, as soon as Mr Manyati ventures out beyond the gates of the premises, he must be guarded and vigilant. Beyond the insults, the threat of jail is real, as Zimbabwe punishes same-sex sexual relationships with up to 14 years imprisonment.
Beyond jail, there is the everyday lived experience of discrimination, violence and hate crimes with which LGBTI people must contend—not only in Zimbabwe, but also in the 69 countries worldwide that criminalize same-sex sexual relationships.
And even in countries that don’t, like neighbouring South Africa. While same-sex marriage is legal and LGBTI rights are constitutionally enshrined, being gay is dangerous. In the first half of 2021, there has been a spate of murders of young gay men and an outcry from the LGBTI community for the government, media and public to take hate crimes more seriously.
Under these conditions, it is an act of defiance just to exist and, even more so, to be deliberately happy.
Happiness is something Mr Manyati has tried to carve out for himself, despite the odds.
Born in Mutoko, a small town in Zimbabwe’s Mashonaland East Province, Mr Manyati says his parents expected him to get married in his twenties to a woman and to carry on the family name as one of the seven Manyati sons.
While his parents insisted on marriage for some time, Mr Manyati stood his ground. As the sole caregiver for his parents and siblings, they eventually gave in and he lived his life single, never coming out to his parents.
“I couldn’t get married because I have the body of a male but, inside, I feel like a female. I know I am … I feel … like a female. So why should I marry a female?”, he says, visibly grappling with complex concepts about his gender identity without the vocabulary to do so.
Here at GALZ, everyone tells him “who they are,” says Mr Manyati. Perhaps with a few more visits and more interaction with the young people around him, who are so much more self-assured in their sexual orientation and gender identity, it may not be too late for Mr Manyati to give name to his feelings.
GALZ is a lifeline for its members. It offers regular clinic days at its Harare drop-in centre and referrals at its other drop-in centres, in Mutare and Masvingo, for a range of health-care services, including HIV prevention and treatment. It also provides critical counselling services and safe spaces for LGBTI people to socialize and relax, away from the “harsh” streets.
The leadership at GALZ says that things are slowly getting better for LGBTI people in Zimbabwe.
In 2017, GALZ was included as an official participant in the funding proposal developed for the Global Fund to Fight AIDS, Tuberculosis and Malaria. This helped to secure US$ 2 million for programmes that serve gay men and other men who have sex with men, the largest investment ever in an HIV and sexual and reproductive health response for the community. The funding resulted in the three GALZ drop-in centres.
The National AIDS Council (NAC) of Zimbabwe has a key populations forum, supported by UNAIDS, and of which GALZ is a member. The NAC is visibly working to improve the health and well-being of key populations even while their activities remain criminalized.
Despite progress, the lingering stigma and discrimination that the LGBTI community faces in Zimbabwe has resulted in Mr Manyati and people of his generation leading an isolated life.
“It makes me feel safer to rather stay by myself,” says Mr Manyati, adding that all his peers and friends from the LGBTI community have since died. “Sometimes I cry,” he sighs.
When Mr Manyati’s friends were alive, they would live their lives to the fullest, even though the law was a constant threat and they remained unlucky in love with the men they encountered.
“[You would know] he doesn't really like you because he has another love somewhere and you are just one on the side. In the end, he gets married and leaves you,” says Mr Manyati of these encounters.
Mr Manyati is adamant that he is “too old” to look for love now, and that he would rather focus on looking after his health as one of the estimated 1.4 million Zimbabweans living with HIV.
Mr Manyati discovered he was living with HIV when he developed a cough five years ago. He went to a local nongovernmental organization, New Start, for an HIV test and after a course of tuberculosis treatment he was initiated immediately onto HIV treatment. His health is his main priority.
“I continue with HIV treatment. That’s how I’m looking healthy now,” Mr Manyati concludes, eyes still shimmering.
* Not Yet Uhuru is a quote by the Kenyan freedom fighter Oginga Odinga. Uhuru is a Swahili word meaning “freedom”; thus, it loosely means “not yet free”. It is a hashtag routinely used by GALZ in its social media posts.
Our work
Region/country
Related
Documents
Community innovations
13 March 2020
This publication is intended to spark interest, inquiry and discussion around community innovations. It draws on the response to the AIDS epidemic—a prime example of disruptive community innovations, not only in the health sector, but with far reaching implications for nearly every aspect of people’s lives—to show that innovation is about enabling communities to have the space, freedom and support to initiate and make changes for themselves. Providing snapshots of innovations across a range of HIV-related themes and geographical areas, this booklet illustrates community innovations through 10 stories on a range of topics, including HIV treatment, mental health issues, tuberculosis (TB) care, service quality, and advocacy to decriminalize consensual same-sex sexual acts. The examples presented here demonstrate both the evolving nature of the challenges faced by an effective HIV response and the ingenuity of the communities that devise ways to overcome them.

Related
 How the shift in US funding is threatening both the lives of people affected by HIV and the community groups supporting them
How the shift in US funding is threatening both the lives of people affected by HIV and the community groups supporting them
18 February 2025
 UNAIDS urges that all essential HIV services must continue while U.S. pauses its funding for foreign aid
UNAIDS urges that all essential HIV services must continue while U.S. pauses its funding for foreign aid
01 February 2025
Impact of community-led and community-based HIV service delivery beyond HIV: case studies from eastern and southern Africa
30 January 2025
 Zambian football star Racheal Kundananji named UNAIDS Goodwill Ambassador for Education Plus in Zambia
Zambian football star Racheal Kundananji named UNAIDS Goodwill Ambassador for Education Plus in Zambia
23 January 2025
A shot at ending AIDS — How new long-acting medicines could revolutionize the HIV response
21 January 2025
 HIV financial data: A transformative power to ensure sustainability of the AIDS response
HIV financial data: A transformative power to ensure sustainability of the AIDS response
19 December 2024
Indicators and questions for monitoring progress on the 2021 Political Declaration on HIV and AIDS — Global AIDS Monitoring 2025
17 December 2024
 To end AIDS, communities mobilize to engage men and boys
To end AIDS, communities mobilize to engage men and boys
04 December 2024